|
Bakteriologisk diagnostik vid urogenitala sjukdomar
Allmänt om bakterieodling vid prostatit Läkartidningen volym 76, nr 21 1979 Nedanstående är ett utdrag av en längre artikel av Dr. Stig Nilsson och där jag återger det väsentligaste: "Olika bakterier ger olika grad av inflammatoriskt engagemang, och storleken därav växlar mellan olika individer. En infektion i prostatakörteln är i allmänhet fokal. Detta begränsar möjligheten att såväl genom massage och experimering av prostatasekret som perineal finspetspunktion och aspiration erhålla representativt materiel för bakteriologisk diagnostik. Den bakteriologiska diagnostiken vid kronisk prostatit bedöms som mycket osäker, dels mot bakgrund av den fokala inflammationen, dels mot bakgrund av att sekret kontamineras under passagen genom uretra. Den kliniska misstanken på infektion kan därför i allmänhet inte styrkas vid rutinmässigt utförd bakteriologisk diagnostik. Graden av kontamination kan reduceras till mer än 50 % genom att patienten omedelbart före massage och exprimering tömmer en fylld urinblåsa. Bedömning av bakteriefyndets signifikans vid odling av prostatasekret är förenad med betydande svårigheter. Valet av transportmedium, förvaringstiden före odling samt temperaturen under transporttiden påverkar möjligheten till bakteriologiska värderingar. Brandberg och medarbetare fann således att vid förvaring såväl vid +4°C som vid +22°C både ejakulatprov och exprimerat sekretprov från bakteriesynpunkt kvantitativt och kvalitativt förändras så genomgripande att provet inte kan bedömas nöjaktigt. Förvaring vid +4°C medför dödande av känsliga bakteriearter. Förvaring vid +22°C kan förutom ett sådant dödande av känsliga bakterier också ge en förskjutning av bakteriefloran, så att vissa arter av såsom exempelvis E. coli och enterokocker kommer att dominera. Konkurrensen mellan bakteriearterna under tillväxten kan medföra att känsligare bakterier reduceras i antal, vilket försvårar isoleringsmöjligheterna av olika förekommande arter. Risken föreligger dessutom att bedömaren låter sig imponeras av kvantiteten av efter olämplig förvaring dominerande bakteriearter. Detta kan sedan vid den kliniska bedömningen medföra att den dominerande bakterien felaktigt tillmäts ha etiologiskt samband med sjukdomen. För att reducera dessa effekter rekommenderas att såväl prov från prostatamassage som ejakulat om möjligt odlas i omedelbar anslutning till provtagningen. Kronisk prostatit är en vanlig orsak till bakteriuri hos yngre och medelålders män. Vid bakteriell prostatit är i allmänhet bakterieantalet i prostatasekret litet, varför negativt odlingssvar erhålls om vanliga kriterier på signifikant bakterieuri tillämpas. Det förefaller inte ovanligt att vid frånvaro av exprimat begära odling på urin som kastats efter massage och exprimat. Detta är en dålig metod som sällan tillåter några konklusioner, främst på grund av den enorma utspädningseffekten och kontamination av uretrafloran. Misstanke om bakteriell prostatit bör alltså verifieras genom kvantitativ bestämning av bakteriearter på prov där exprimerat sekret direkt strukits på odlingsplatta eller samlats i buljongrör."
Tillbaka till Appell till den svenska sjukvården
Mycoplasma genitalium and Chlamydia trachomatis Comparison of first void urine and urogenital swab specimens for detection of Mycoplasma genitalium and Chlamydia trachomatis by polymerase chain reaction in patients attending a sexually transmitted disease clinic. Jensen JS, Bjornelius E, Dohn B, Lidbrink P. Mycoplasma Laboratory, Department of Respiratory Infections, Meningitis, and Sexually Transmitted Infections, Statens Serum Institut, Copenhagen S, Denmark. jsj@ssi.dk OBJECTIVE: The objective of this study was to compare urogenital swab specimens and first void urine (FVU) specimens from male and female patients at a sexually transmitted disease clinic for the detection of Mycoplasma genitalium and Chlamydia trachomatis infections using in-house, inhibitor-controlled polymerase chain reaction (PCR). STUDY DESIGN: Urethral swabs and FVU were collected from 1856 men and 753 women who also had a cervical swab collected. A positive diagnosis of infection was made if any 1 of the specimens tested positive and were confirmed in a second PCR assay targeting independent genes. RESULTS: M. genitalium DNA and C. trachomatis DNA were detected in 126 (6.8%) and 246 (13.3%) of the male sample sets and in 51 (6.8%) and 73 (9.7%) of the female specimen sets, respectively. Using our in-house PCR and sample preparation methods, FVU was found to be the most sensitive diagnostic specimen for both pathogens, but for optimal sensitivity, it should be supplemented with a cervical specimen in women. In a small subset of female FVUs, storage at -20 degrees C led to false-negative M. genitalium PCR results in 27% of specimens found positive when a sample preparation was performed before freezing. The age-specific prevalence of M. genitalium in men was almost constant between 18 and 45 years of age in contrast to C. trachomatis infections, which were more common in younger men. CONCLUSION: Urine appeared to be a better diagnostic specimen than the urethral swab for M. genitalium and C. trachomatis detection by PCR in this cohort of sexually transmitted disease clinic attendees but should be supplemented with a cervical specimen in women. PMID: 15273584 [PubMed - indexed for MEDLINE] Om behandlingsresultat av kronisk prostatit och jämförelse av sjukdomarna, se följande rubrikern på sidorna Statistik/historik och Svensk forskning: Comparative analysis of azithromycin and clarithromycin , Azithromycin and Ofloxacin Found to be Most Active against Chlamydia in Men with Chronic LowerUrinary Tract Symptoms och Symptomatic urethritis is more prevalent in men infected with Mycoplasma genitalium than withChlamydia trachomatis
Current Methods of Laboratory Diagnosis of Chlamydia trachomatis Infections CLINICAL MICROBIOLOGY REVIEWS, Jan. 1997, p. 160-184 Vol. 10, No. 1 CAROLYN M. BLACK* Division of AIDS, Sexually Transmitted Diseases, and Tuberculosis Laboratory Research, National Center for Infectious Diseases, Centers for Disease Control and Prevention, Atlanta, Georgia 30333 Serologic tests are generally not useful in the diagnosis of genital tract infections caused by C. trachomatis. This is because antibodies elicited by C. trachomatis infection are long lived and a positive antibody test will not distinguish a previous from a current infection. The use of convalescent-phase serum specimens can be helpful, since a fourfold increase in antibody titer is predictive of an active infection; however, it can take up to 1 month or longer for antibody titers to rise, and the delay is not appropriate to the time frame necessary for therapy and management of patients. The presence of IgM antibodies is an unreliable marker of acute infection in adolescents and adults since IgM is often not present, presumably because the person has been infected previously with C. trachomatis or possibly with another chlamydial species such as C. pneumoniae and is generating an anemnestic response to the most recent exposure. In spite of test manufacturers' claims, no currently available serologic test of a single serum specimen will provide conclusive evidence of current infection with C. trachomatis posure of the individual.
Dr. Sandra Mazzoli's forskning angående diagnosticering av Chlamydia, Italien. Som framgår av ovanstående artikel ("Current Methods.....") anses de nuvarande tillämpade metoderna för diagnos av Chlamydia trachomatis som otillförlitliga. Vi hänvisar därför till en undersida med Dr. Sandra Mazzolis senaste forskningsrön angående vilka laboratoriemetoder som hon avänder och som hon anser vara mycket tillförlitligare. Du når undersidan genom att klicka på Dr. Sandra Mazzoli.
Odling av ejakulat enligt E.N. På remissen, som skrivs ut av läkaren, skall det stå utvidgad spermieodling och att den skall behandlas inom en timma (åk till labbet själv). Du får inte ha haft utlösning på minst 5 dagar. Börja med att kissa och tvätta därefter ollonet noga. Onanera i ett rent glas/plastmugg eller annat lämpligt föremål och för över innehållet försiktigt i ett provrör (sterilt provrör erhåller du samtidigt som remissen). Om det inte går att hälla över så använd en spruta (får köpas på Apotek utan kanyl) och sug upp och för över i provröret. Förvara provet intill kroppen (tejpa t.ex. fast provet i en armhåla) och ”kila iväg” till labbet så snabbt som möjligt utan att utsätta provet för temperaturväxlingar. Påpeka för personalen att det står på remissen att provet skall behandlas inom 1 timme och med hänsyn till din restid måste dom därför behandla provet omgående. I Göteborg är det Bakteriologen vid Sahlgrenska Universitetssjukhuset som tar hand om dessa prover.
Diagnostic Test Philosophy (IC)Av Dr. Paul Fugazzotto. http://luna.moonstar.com/~crc/drf.html. Se även: http://www.moonstar.com/~icickay/articles/therearenowtwo.pdf It is very likely you are not acquainted with me and my work on urinary tract infections. I have been a diagnostic and research microbiologist since 1938, and I think my half century of experience gives me an edge in this area of research. The medical community has long been educated to the idea that urinary tract infections (UTI) are by some mystic aura different from other infections, and has been convinced that the numbers of organisms found (any species at all) is diagnostic of infection. In other infections, the diagnosis depends on finding the specific respective organism, irrespective of numbers: i.e.: a darkfield exam of a suspected chancre need produce just one typical Treponome, and you have undeniable proof of Syphilis: just ONE among millions of contaminants! Specific pathogens prove the diagnosis. My approach to UTI and Interstitial Cystitis (IC) is the same as for any other infections: using well established classical procedures. Dr. Fugazzotto believes that the urine and pelvic screening tests in widespread use everywhere cannot give an accurate result for a large number of patients. They are based on layman concept of "colony counts". In this concept, you must have a high amount of bacterial growth in a specific period of time to be classified as having a UTI. He sees many problems with this approach.
Doctors and patients alike must insist that the "colony count" practice be immediately discontinued, and that medical labs learn and adopt the only valid approach to evaluation of pelvic infection: Pure culture technology (which requires initial culture of specimens in broth, to allow all microbial strains from the specimens to emerge). Then by transfer of aliquots to appropriate differential media, the etiologic agent can be isolated for further study, and be reported to the attending physician along with the appropriate antibiotic sensitivity pattern. Plus, the physicians' prescriptions no longer becomes a hit and miss proposition. ISOPs anm: Ovanstående resonomang gäller givetvis i lika hög grad för kronisk prostatit.
Tillbaka till Bakteriologisk diagnostik vid IC (På sidan Interstitiell cystit (IC))
Sampling protocol for chronic prostatitis. Sex abstinence for at least three days before sampling. No antibiotic for at least 1 week before sampling. Bugs present in the whole genital tract:
To better differentiate prostatic germs:
All these samples will be analysed for the presence of all common bacteria, yeasts, urogenital mycoplasmata, DNA of Chlamydia trachomatis, Neisseria gonorrhoeae, HPV, and additionally for specific Chlamydia t. secretory IgA, that represents a good local marker of infection. The results will also be confirmed by Electron Microscopy. Sandra Mazzoli, PhD, S.T.D. Centre Responsible, Sexually Transmitted Disease Centre, Santa Maria Annunziata Hospital, Via dele Antella 58-Antella, Florence, Tuscany 50111, Italy, Tel: +39-055-2496459, Fax: +39-055-2496459 Email: s.mazzoli@mclink.it
Bacterial Cultures in urine, prostatic fluid and semen of men with Chronic Pelvic Pain Syndrome: Role of culture for 2 vs 5 days, USA. Daniel A. Shoskes, Carissa Mazurick, Richard Landis, Michael Ruggieri, Robert B. Nadler, Keith Jarvi, Lee Nyberg, NIH Chronic Prostatitis Collaborative Research Network Torrance, CA; Philadelphia, PA; Chicago, IL; Toronto, ON, Canada; Washington, DC. Introduction: The role of bacterial pathogens in chronic pelvic pain syndrome (CPPS) is controversial. Nevertheless, some patients do respond well to antibiotic therapy despite negative cultures. Prostatic fluid (EPS) may require longer culture duration to detect bacterial growth than the 2 days commonly used for urine. We wished to compare 2 and 5 days of culture for bacterial detection in EPS and urine. Conclusions: By culturing EPS or semen for 5 days rather than 2 days, an additional 7.5% will be found positive for bacteria that localize to the prostate. Gram-positive bacteria found this way are associated with increased inflammation in EPS.
The only way in which the diagnosis of prostatitis can be objective established is by microscopy of expressed prostatic fluid together with quantitative bacteriologic cultures of specimens from urethra and the bladder and from EPS/expressed prostatic secretion. Ovanstående enligt Dr. Stig Colleen (urolog) och Dr. Per-Anders Mårdh (mikrobiolog). Från "Sexually Transmitted Diseases" i kapitel 54 med början på sidan 653. Utgiven på förlag McGraw-Hill, Inc 1990. ISBN 0-07-029677-4. Mer utdrag hittar du på undersidan Laboratory Diagnosis.
Insamling av urin och prostatasekret för laboratorieanalys enligt läkemedelsföretaget Astra-Zeneca http://www.astrazeneca.ch/fr/index/urologie/prostata-andere/prostatitis/prostatitis-aufbau.htm
Microscopic and microbiological findings for evaluation of chronic prostatitis Reference: Magri V, Cariani L, Bonamore R, Restelli A, Garlaschi MC, Trinchieri A. in Arch Ital Urol Androl. 2005, Jun;77(2):135-8. Examination of the urine after prostatic massage is beneficial in patients with prostatitis; according to a recent study. An Italian study has concluded that microscopic examination of urine after prostatic massage is a feasible indicator of prostatic inflammation. The study, called “Microscopic and microbiological findings for evaluation of chronic prostatitis,” by Magri et al., in the Archives of Italian Urology and Andrology, covered 233 patients with symptoms suggesting prostatitis, but who did not have urethral discharge. The same urologist evaluated all the patients by performing a medical history, physical examination, and transrectal ultrasound. The study said 47% of the 233 patients had a positive urethral culture, 35% a positive culture of the seminal fluid and 13% had a positive culture of one or more samples of the four-specimen localization test. According to the study, more than 10 leukocytes in the post-massage urine were observed in 49% of patients with a positive culture of the seminal fluid.
I have discussed the microbial investigation of prostatitis many times on the BPSA site and stressed the importance of not only having "good" microbiology but also, expert interpretation of the microscopy of the various samples produced. However, within the NHS this type of investigation is poorly understood and the methods used in these laboratories do not reflect the requirements of such specimens. This service "The Stamey Localisation Method" is available privately and I have been providing it for about 20+ years. Dr. Simon Rattenbury, UK. Email: srattenbury@yahoo.ie
Urinalysis: A Comprehensive Review En omfattande artikel från den 15 mars 2005 om urinanalys finns för nedladdning från American Academy of Family Physicians på http://www.aafp.org/afp/20050315/1153.html och http://www.aafp.org/afp/20050315/1153.pdf . Författare är JEFF A. SIMERVILLE, M.D., WILLIAM C. MAXTED, M.D., and JOHN J. PAHIRA, M.D.
Metoden beskrivs på undersidan PCR/RNA-teknik. Detta är en metod som bygger på att man identifierar bakterier genom dess 16S ribosomal RNA. RNA is a nucleic acid molecule similar to DNA but containing ribose rather than deoxyribose. RNA is formed upon a DNA template. There are several classes of RNA molecules. They play crucial roles in protein synthesis and other cell activities. Denna metod anses väl lämpad vid undersökning av urogenitala sjukdomar, då man genom andra metoder inte kunnat fastställa sjukdomsorsaken. Oss veterligt används PCR-tekniken än så länge inom svensk sjukvård vid urogenitala sjukdomar, endast då man misstänker att sjukdomsorsaken är Chlamydia trachomatis eller Mycoplasma genitalium?
Panfungal PCR and Multiplex Liquid Hybridization for Detection of Fungi in Tissue Specimens J Clin Microbiol 2000 Nov;38(11):4186-4192 Related Articles, Books, LinkOut Hendolin PH, Paulin L, Koukila-Kahkola P, Anttila VJ, Malmberg H, Richardson, M, Ylikoski J.'Institute of Biotechnology, University of Helsinki, 00014 University of Helsinki. [Record supplied by publisher] A procedure based on panfungal PCR and multiplex liquid hybridization was developed for the detection of fungi in tissue specimens. The PCR amplified the fungal internal transcribed spacer (ITS) region (ITS1-5.8S rRNA-ITS2). After capture with specific probes, eight common fungal pathogens (Aspergillus flavus, Aspergillus fumigatus, Candida albicans, Candida krusei, Candida glabrata, Candida parapsilosis, Candida tropicalis, and Cryptococcus neoformans) were identified according to the size of the amplification product on an automated sequencer. The nonhybridized products were identified by sequencing. The performance of the procedure was examined with 12 deep-tissue specimens and 8 polypous tissue biopsies from the paranasal sinuses. A detection level of 0.1 to 1 pg of purified DNA (2 to 20 CFU) was achieved. Of the 20 specimens, PCR was positive for 19 (95%), of which 10 (53%) were hybridization positive. In comparison, 12 (60%) of the specimens were positive by direct microscopy, but only 7 (35%) of the specimens showed fungal growth. Sequencing of the nonhybridized amplification products identified an infecting agent in six specimens, and three specimens yielded only sequences of unknown fungal origin. The procedure provides a rapid (within 2 days) detection of common fungal pathogens in tissue specimens, and it is highly versatile for the identification of other fungal pathogens. PMID: 11060088
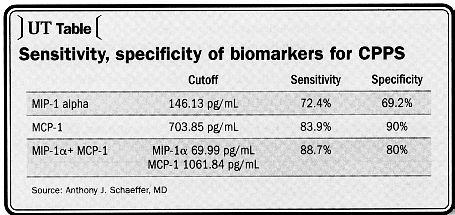
Dr. Anthony J. Schaeffer, MD. Northwestern School of Medicine, Chicago. Reprint from Urology Times, August 15, 2005. A study from Dr. Schaeffer's own lab identified two new biomarkers in expressed prostatic secretions that appear not only to have a high degree of sensitivity and specificity for CPPS, but may also shed light on the pathogenesis of the disease. The cytokine macrophage inflammatory protein-lalpha (MIP-1α has a sensitivity of 72.4% and a specificity of 69.2%; monocyte chemoattractant protein-1 (MCP-1) has a sensitivity of 83.9% and a specificity of 90%. Combined, the two have a sensitivity of 88.7% and a sensitivity of 80%. "Men with CCPS frequently have prostatic inflammation. This study indicates that they also have these two elevated cytokines. These may, in fact, be biomarkers for the disease. Further study is needed to determine how these biomarkers are modulated during the course of the disease and if treatment with anti-cytokines might be warranted," Dr. Schaeffer said.
Olika forskare hävdar att EPS är att föredra framför ejakulat, oavsett vilken diagnosmetod som används. Detta antagande bygger troligtvis på, att en inflammerad prostata inte klarar av att pressa ut inkapslat sekret (ev. innehållande patogena bakterier) vid en normal sädestömning.
Laboratorieodling av bakterier i Petriskål.
Tillbaka till Diagnos (på sidan Prostatasjukdomarna)
|