|
Eventuella samband mellan olika prostatasjukdomar
Epidemiology of prostatitis: new evidence for a world-wide problem. Krieger JN, Riley DE, Cheah PY, Liong ML, Yuen KH. Department of Urology, University of Washington School of Medicine, VAPSHCS (112-GU), 1600 South Columbian Way, Seattle, WA 98108, USA. World J Urol 2003 Apr 24 Från
denna medicintidskrift saxar jag följande av intresse:
Augusti 2007. Wang W, Bergh A, Damber JE Department of Urology, Lundberg Laboratory for Cancer Research, The Sahlgrenska Academy at Göteborg University, Göteborg, Sweden. BACKGROUND: Proliferative inflammatory atrophy (PIA) in the prostate has been proposed to be a precursor to prostate cancer. CCAAT/enhancer-binding protein beta (C/EBPbeta) is an important transcription factor involved in cellular proliferation and differentiation. Activation of C/EBPbeta plays a crucial role during the initial stage of cyclo-oxygenase 2 (COX-2) induction by proinflammatory mediators. Overexpression of C/EBPbeta has been reported in several human tumors. Nevertheless, the C/EBPbeta expression and functions in human prostate tissue are basically unknown. METHODS: C/EBPbeta immunohistochemical staining was performed on 45 benign prostate hyperplasia (BPH) samples. The expression of C/EBPbeta in PIA lesions and normal-appearing acini was analyzed. In addition, by using double-IHC staining, C/EBPbeta expression and the association with chronic inflammatory cell density, co-expression of COX-2 and androgen receptor (AR) were also investigated. RESULTS: C/EBPbeta was occasionally observed in normal-appearing prostate acini (4.9% +/- 6.7%, Mean +/- SD) but was clearly overexpressed in PIA lesions (81.8% +/- 16.4%) (P < 0.0001). Atrophic glands with T-lymphocyte and macrophage inflammation expressed higher level of C/EBPbeta. Furthermore, C/EBPbeta correlated significantly with COX-2 expression. Downregulation of the AR was common in PIA and was also related to the C/EBPbeta overexpression. CONCLUSIONS: The data demonstrated that chronic inflammation appeared to play roles in the induction of C/EBPbeta expression in prostate epithelium, which was in turn associated with increased COX-2 expression and AR downregulation. In combining with other molecular alteration in the epithelium of PIA, it is suggested that these cells might be a kind of intermediate cells and involved in the pathogenesis of prostate cancer. (c) 2007 Wiley-Liss, Inc. PMID: 17570496 [PubMed - indexed for MEDLINE]
Chronic Prostatic Inflammation May Fuel Carcinogenesis: Study 2006-04-05 By Megan Rauscher WASHINGTON (Reuters Health) - Chronic inflammation of the prostate may significantly raise the risk of prostate cancer, according to a study presented here this week at the 97th annual meeting of the American Association for Cancer Research, http://www.aacr.org. This work was was led by Sanjay Gupta, Ph.D., assistant professor of urology at Case Western Reserve University in Cleveland, along with Greg MacLennan, M.D., associate professor of pathology. Study presenter Dr. Sanjay Gupta from Case Western Reserve University in Cleveland noted that an association between inflammation and some types of cancer has been established, but whether chronic prostatic inflammation contributes to the development of prostate cancer is unclear. To investigate, he and colleagues determined the presence and extent of inflammation in 177 initial and follow-up needle prostate biopsies from men with clinical parameters suspicious for malignancy. The men had abnormal serum PSA levels and/or digital rectal exams. Of the 177 initial biopsies, chronic inflammation was observed in 144 (81%). Twenty-nine (20%) of the initial biopsies with chronic inflammation showed adenocarcinoma compared with 10 (30%) of the 33 initial biopsies without inflammation. In 84 subsequent biopsies obtained within 5 years from patients who initially showed chronic prostate inflammation, 29 new prostate cancers were diagnosed (35%). "In sharp contrast," Dr. Gupta said, there were only two new cases of adenocarcinoma (6%) in the 33 men without inflammation on the initial biopsy. As expected, there was a significant correlation between serum PSA level and inflammation grade. "From these data, we can conclude that a strong association exists between chronic prostatic inflammation and the development of premalignant and malignant tumors in prostate epithelia," Dr. Gupta told meeting attendees. These results prompt two questions, he added. "First, should patients whose initial biopsies showing no malignancy but chronic inflammation be followed more closely or perhaps re-biopsied? And second, is it wise to recommend watchful waiting for patients with low-grade adenocarcinoma that is accompanied by chronic inflammation?" Studies designed to help "substantiate these findings and help resolve these questions" are planned, he said. Se: http://urotoday.com/prod/contents/prostatitis/article.asp?cat=prostatitis&sid=&tid=&aid=4469
Inflammation and Atrophy in Prostate Carcinogenesis The American Urological Association (AUA)'s Annual Meeting is the largest meeting of urologic professionals in the world. With more than 10,000 urologists and health-care professionals and 5,000 exhibitors in attendance, there is no better place to learn about the latest advances in urology. Mötesplats 2006: Den 20-25 maj i Atlanta, Georgia,USA. Huvudsida http://www.aua2006.org/am06/ På http://webcasts.prous.com/Aua2006/article.asp?AID=30&CID=YY&CLID=2 finns en förteckning över Webcasts från årets möte. Bl.a. finns en föreläsning om samband mellan inflammation (kronisk prostatit) och en ev. senare utveckling av prostatcancer. Under Webcast Program klicka på Inflammation and Atrophy in Prostate Carcinogenesis, Angelo M. De Marzo, M.D., Ph.D. Department of Pathology, The Johns Hopkins University School of Medicine, Baltimore, Maryland och därefter på Proceed to Webcast och välj aktuell internetuppkoppling. Här anges inledningsvis att minst 20 % av ALL cancer är en följd av en infektion och/eller inflammation.
Anm
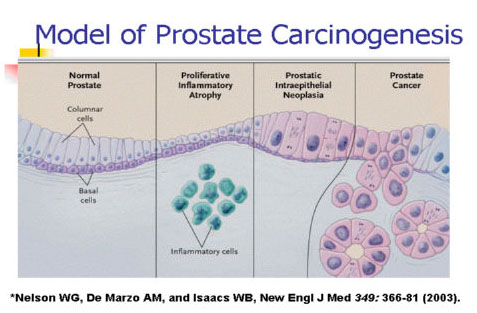
(se ovanstående bild):
How
inflammation can lead to cancer (bild 12 i ovanstående Webcast):
Monday, 15 March 2010 BERKELEY, CA (UroToday.com) - Recent studies have shown a highly suggestive correlation between prostatitis, chronic inflammation, and the diagnosis of PCa (1). An important issue is the improvement of prostate imaging with new strategies in order to define both vascular and metabolic pattern changes in inflammation, HGPIN, and cancer lesions. Recently, a large number of studies (2-4) have shown that the addition of proton 1H-magnetic resonance spectroscopic imaging (1H-MRSI) and dynamic contrast-enhanced magnetic resonance (DCE-MRI) could represent a powerful tool for the early diagnosis of PCa. Normal prostate tissue contains normal levels of Citrate (Cit) and low Choline (Cho) levels, while an increase in Cho levels is seen in regions with prostate carcinoma (5-6). Despite normal epithelial cells, the ability to generate and concentrate Cit is expected to be lost in cancer cells (7). Moreover the elevated Cho peak reflects an elevated cell proliferation rate. We investigated changes in 1H-MRSI and DCE-MRI parameters from histologically confirmed prostatic inflammation, HGPIN, low-grade prostate cancer (LGPCa), and high-grade prostate cancer (HGPCa). All cases included in this study were submitted to a TRUS guided prostate biopsy within 2 weeks after an MR imaging research protocol that was implemented at our Institution. 1H-MRSI and DCE-MRI procedures were carried out for the diagnosis and localization of cancer within the prostate gland. The protocol included all patients who were selected for a prostate biopsy, on the basis of an increased serum PSA level (greater than 4 ng/mL) with a normal digital rectal examination (DRE). Exclusion’s criteria were: clinical diagnosis of acute prostatitis, coexistent clinically proven cancer, hormonal therapies (including 5 alpha reductase inhibitors), radiotherapy, chemotherapy, previous surgery on the prostate gland, cases in which was not possible complete MR’s study with 1H-MRSI, and DCE-MRI. Patients who do not fit these criteria were excluded. MR images were analyzed in consensus by two radiologists with 9 and 3 years of experience in urogenital MRI. They were unaware of initial PSA serum levels and TRUS-biopsy results. Similarly to other experiences (8), to obtain a better comparison between MR and pathologic data, the peripheral zone of the prostate was divided in sextant and biopsy targeting was done in zones corresponding to those analyzed with 1H-MRSI and DCE-MRI. No analysis in the transitional zone of the prostate was performed. Ninety-six men were selected and were divided in a control group, Group A, with no evidence of prostate disease, Group B with diagnosis of chronic inflammation, Group C high grade (HG) PIN Group D with low grade prostate cancer (LGPCa) and Group E with high grade Prostate cancer (HGPCa). At MRSI, the quantitative analysis of individual metabolites concentration showed significant differences between controls and the other groups and similar patterns among inflammation, HGPIN and LGPCa. In particular, the analysis of Cho concentration showed very similar (p >.05) levels among inflammation, HGPIN, and LGPCa, all significantly higher (p < .05) than control and significantly (p < .05) lower than HGPCa. In our study the similar levels of Cho among inflammation, HGPIN, and LGPCa, all higher than controls but lower than HGPCa, may suggest a correlation or a potential evolutionary trend among these lesions. The results of the ratio analysis confirmed a correlation between inflammation and HGPIN but showed no significant differences (p > .05) between LGPCa and HGPIN. Our findings demonstrate significant differences among normal prostate tissue, chronic inflammation, HGPIN, and cancer and associations with 1H-MRSI patterns, which suggest that we did correctly localize the different lesions. No final conclusions can be made from our study, but our results suggest the potential for these MR imaging techniques in the description of inflammatory and proliferative lesions inside the prostate gland. References: 1. Sciarra, A.; Di Silverio, F.; Salciccia, S.; Autran Gomez, A.M.; Gentilucci,A.; Gentile, V. Inflammation and chronic prostatic diseases: evidence for a link? Eur Urol 2007 Oct, 52(4), 964–972. 2. Mazaheri, Y.; Shukla-Dave, A.; Hricak, H.; Fine, S.W.; Zhang, J.; Inurrigarro, G.; Moskowitz, C.S.; Ishill, N.M.; Reuter, V.E.; Touijer,K.; Zakian, K.L.; Koutcher, J.A. Prostate cancer: identification with combined diffusion-weighted MR imaging and 3D 1H MR spectroscopic imaging-correlation with pathologic findings. Radiology 2008 Feb, 246(2), 480–488 3. Sciarra, A.; Salciccia, S.; Panebianco, V. Proton spectroscopic and dynamic contrast-enhanced magnetic resonance: a modern approach in prostate cancer imaging. Eur Urol 2008, 54(3), 485–488. 4. Kumar, R.; Nayyar, R.; Kumar, V.; Gupta, N.P.; Hemal, A.K.; Jagannathan, N.R.; Dattagupta, S.; Thulkar, S. Potential of magnetic resonance spectroscopic imaging in predicting absence of prostate cancer in men with serum prostate-specific antigen between 4 and 10 ng/mL: a follow-up study. Urology 2008, 72(4) 859–863. 5. Testa, C.; Schiavina, R.; Lodi, R.; Salizzoni, E.; Corti, B.; Farsad, M.; Kurhanewicz, J.; Manferrari, F.; Brunocilla, E.; Tonon, C.; Monetti, N.; Castellucci, P.; Fanti, S.; Coe,M.; Grigioni,W.F.; Martorana, G.; Canini, R.; Barbiroli, B. Prostate cancer: sextant localization with MR imaging, MR spectroscopy, and 11C-choline PET/CT. Radiology 2007 Sep, 244(3), 797–806. 6. Palapattu, G.S.; Sutcliffe, S.; Bastian, P.J.; Platz, E.A.; De Marzo, A.M.; Isaacs, W.B.; Nelson, W.G. Prostate carcinogenesis and inflammation: emerging insights. Carcinogenesis 2005 Jul, 26(7), 1170–1181. 7. Noworolski, S.M.; Vigneron, D.B.; Chen, A.P.; Kurhanewicz, J. Dynamic contrast-enhanced MRI and MR diffusion imaging to distinguish between glandular and stromal prostatic tissues. Magn Reson Imaging 2008, 26(8), 1071–1080. 8. Wefer, A.E.; Hricak, H.; Vigneron, D.B.; Coakley, F.V.; Lu, Y.;Wefer, J.; Mueller-Lisse, U.; Carroll, P.R.; Kurhanewicz, J. Sextant localization of prostate cancer: comparison of sextant biopsy, magnetic resonance imaging and magnetic resonance spectroscopic imaging with step section histology. J Urol 2000 Aug, 164(2), 400–404. Written
by: 1Department of Urology, 2 Department of Radiology, Sapienza University of Rome, Italy. The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Prostate cancer linked to infection Sunday, 15 September, 2002, 23:20 GMT 00:20 UK http://news.bbc.co.uk/2/low/health/2254320.stm Scientists have pinpointed a gene that appears to play an important role in the development of prostate cancer.The gene - known as MSR1 - has already implicated in hardening of the arteries associated with heart disease. The findings suggest that at least some cases of prostate cancer may begin with an infection and inflammatory response. " It may tie infections to cancer of the prostate in a way that we haven't thought about before ". MSR1 helps immune system cells called macrophages clean up cellular debris from bacterial infections and damaged fats. Macrophage activity has been known to increase in the early stages of prostate cancer. Scientists suspect that some MSR1 mutations might inhibit the ability of macrophages to clean up properly after prostate infections, leading to damage that may lead to cancer. MutationsResearchers from Wake Forest University and Johns Hopkins Medical School examined men from Caucasian and Afro-Caribbean decent to find out what percentage carried specific mutations of the gene. They found that one type of mutation was present in 4.4% of Caucasians with prostate cancer, compared to just 0.8% who were free from the disease. A different mutation of the gene was found in 12.5% of African-American men with prostate cancer, compared to 1.82% of unaffected men. The researchers believe that MSR1 will prove to be just one of a number of genes linked to prostate cancer. However, it does appear to play a significant role in the developmentof the disease. Researcher Professor William Isaacs said: "This is the first time that MSR1 has been linked to cancer, and it may tie infections and similar environmental exposures to cancer of the prostate in a way that we haven't thought about before." Dr Simon Gamble, of the Prostate Cancer Charity, said it was crucial to find genes that played a role in hereditary prostate cancer if scientists were to fully understand how the cancer grows in the body. He told BBC News Online: "Using the information on the known MRS1 gene mutations and a reliable screening programme it may be possible to observe people with these mutations more closely and diagnose their cancer in the early stages, meaning that their chances of survival will be much higher. "Secondly, the identification of a mutation in the MSR1 gene which makes the cancer spread more rapidly is very important in tailoring treatment to the individual patient. "Patients with this gene mutation can now be identified and could therefore be treated with a stronger treatment regime than those who do not have the mutation." However, Dr Gamble said many prostate cancers were not hereditary, and doubtless there were many more genes yet to be discovered which had an influence on prostate cancer formation in those non-hereditary cases. The research is published in the journal Nature.
CP/CPPS and Prostate Cancer Don’t Share Genetic Variation Ki Hak Song, Seattle, WA, Donald E Riley, Teresa L Gilbert, In Rae Cho, Ilsan, Republic of Korea, Young Seop Chang, Daejeon, Republic of Korea, John N Krieger, Seattle, WA Do androgen receptor polymorphisms contribute to an increased risk for chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) and prostate cancer (CaP)? Because male hormones (androgens) influence prostate growth and because inflammation may be implicated in cancer development, these researchers looked at whether some genetic variation related to androgens might predispose men to chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS), prostate cancer, or both. They looked short tandem repeats (STRs) at the androgen receptor gene in 63 CP/CPPS patients, 88 prostate cancer patients, and 72 control men. STRs are short repeats of DNA that help identify variations in a gene. CP/CPPS patients and prostate cancer patients had distinct and typical variations at the androgen receptor that were different from controls but also different from each other. Some change in the androgen receptor, concluded the researchers, might predispose a man to one condition or the other, but the specific variations and the disease mechanisms likely differ.
Does Bacterial-induced Inflammation Play a Role in Prostate Cancer? Cohen RJ, Shannon BA, McNeal JE, Shannon T, Garrett KL Propionibacterium acnes associated with inflammation in radical prostatectomy specimens: a possible link to cancer evolution? J Urol. 2005 Jun;173(6):1969-74 These Australian researchers cultured microorganisms from the prostate tissue taken out during radical prostatectomy for prostate cancer. The team also looked at the tissue microscopically for inflammation. The most common organism they detected was a type of bacteria known as Propionibacterium acnes, which they found in 35% of the prostate samples. Also, they saw significantly more inflammation in the prostate tissue from men who had P acnes than men who didn’t. They found that the P acnes bacteria in prostate tissue had characteristics that are different from the P acnes normally found on skin. The researchers suggested that these bacteria may be involved in the inflammation they saw and possibly in prostate cancer itself.
Prostatitis as a risk factor for prostate cancer Epidemiology. 2004 Jan;15(1):93-9. Roberts RO, Bergstralh EJ, Bass SE, Lieber MM, Jacobsen SJ. Department of Health Sciences Research, Division of Epidemiology, Mayo Clinic, Rochester, Minnesota 55905, USA. roberts.rosebud@mayo.edu BACKGROUND: The association of infection or inflammation of the prostate with prostate cancer has been suggested but not established. This study was undertaken to investigate this association. METHODS: Cases were Olmsted County, Minnesota, residents with histologically proven prostate cancer diagnosed between January 1980 and December 1996. Cases (n = 409) were each matched to 2 control subjects (n = 803) on age at diagnosis of prostate cancer, residency in Olmsted County, and duration of the community medical record. The medical record of each subject was reviewed for a history of acute or chronic bacterial prostatitis or chronic pelvic pain syndrome (inflammatory type). RESULTS: The relative odds of prostate cancer were elevated in men with history of any type of prostatitis (odds ratio [OR] = 1.7; 95% confidence interval [CI] = 1.1-2.6) or acute prostatitis (2.5; 1.3-4.7). The mean time from most recent episode of acute prostatitis to the diagnosis of prostate cancer was 12.2 years. After exclusion of men with acute prostatitis 2 years before the index date, the relationship was somewhat reduced (1.9; 0.9-3.8). Chronic bacterial prostatitis was more weakly associated with prostate cancer (1.6; 0.8-3.1), whereas chronic pelvic pain syndrome was not associated at all (0.9; 0.4-1.8). CONCLUSIONS: Infection in the form of acute or chronic bacterial prostatitis may be associated with prostate cancer. However, our data do not provide compelling evidence to support this. As a result of the limitations of current methods of assessing chronic prostatitis, biochemical or tissue markers of infection or inflammation of the prostate may help clarify their role in the pathogenesis of prostate cancer. PMID: 14712152 [PubMed - in process]
The role of inflammation in the pathogenesis of prostate cancer Journal
of Urology. Innovations and Challenges in Prostate Cancer: Prevention, Detection
and Treatment: Fourth International Conference. 172(5, Part 2 of 2)
Supplement:S6-S12, November 2004. Abstract: Purpose: A new hypothesis for the etiology of prostate cancer is that chronic or recurrent prostate inflammation may initiate and promote prostate cancer development. Materials and Methods: We reviewed the current direct and indirect evidence from epidemiology, genetics, molecular biology and histopathology implicating inflammation in the pathogenesis of prostate cancer. Results: The case for prostate inflammation as a cause of prostate cancer is compelling. Epidemiology data have correlated prostatitis and sexually transmitted infections with increased prostate cancer risk and intake of anti-inflammatory drugs and antioxidants with decreased prostate cancer risk. Genetic studies have identified RNASEL, encoding an interferon inducible ribonuclease, and MSR1, encoding subunits of the macrophage scavenger receptor, as candidate inherited susceptibility genes for familial prostate cancer. Somatic silencing of GSTP1, encoding a glutathione S-transferase capable of defending against oxidant cell and genome damage, has been found in almost all prostate cancer cases. Proliferative inflammatory atrophy lesions containing activated inflammatory cells and proliferating epithelial cells appear likely to be precursors to prostatic intraepithelial neoplasia lesions and prostatic carcinomas. Conclusions: Emerging hints that prostate inflammation may contribute to prostatic carcinogenesis will provide opportunities for the discovery and development of new drugs and strategies for prostate cancer prevention. Copyright (C) 2004 by American Urological Association, Inc.
Periglandular chronic inflammation Stephen B. Strum MD, FACP. Medical Oncologist Specializing in Prostate Cancer. From http://www.prostatepointers.org RE: [p2p] Periglandular Chronic Inflammation. August 2005. "Periglandular chronic inflammation means that there were cells associated with inflammation seen surrounding some of the typical glandular formations which are part of the histologic appearance of prostate tissue. This may be related to prostatitis. Many believe that prostatitis is a co-factor in the development of prostate cancer.
Samband
enligt Prof. Bernard Lobel, Centre
Hospitalier Universitaire de Rennes, Frankrike.
Human prostate cancer precursors and pathobiology Urology. 2003 Nov;62(5 Suppl 1):55-62. De Marzo AM, Meeker AK, Zha S, Luo J, Nakayama M, Platz EA, Isaacs WB, Nelson WG. Department of Pathology, The Johns Hopkins University School of Medicine, Baltimore, Maryland 21231-1000, USA. ademarz@jhmi.edu Prostate cancer is among the most common malignancies. It is estimated that 1 in 6 men in the United States will be diagnosed with this disease. Despite the high prevalence and importance of prostate cancer, the molecular mechanisms underlying its development and progression remain poorly understood. This article reviews new information about the roles of oxidants and electrophiles in prostate cancer; the potential importance of chronic inflammation and atrophy in prostate carcinogenesis, and implications for chemoprevention; evidence supporting telomere shortening and genetic instability in the etiology of prostate cancer; and alpha-methylacyl-coenzyme A racemase (AMACR) as a potential marker for prostate carcinogenesis. These new results show that at least some high-grade prostatic intraepithelial neoplasias (PIN) and early adenocarcinomas appear to arise from proliferative inflammatory atrophy (PIA). Inflammation and other environmental factors may lead to the destruction of prostate epithelial cells, and increased proliferation may occur as a response to this cell death. Such proliferation may be mechanistically related to decreased p27(Kip1) observed in PIA. The decreased apoptosis associated with these events may also be related to increased expression of Bcl-2. Increased oxidant and electrophile stress in the setting of increased proliferation associated with these events may lead to elevated glutathione S-transferase P1 (GSTP1) expression as a genomic-protective measure. However, aberrant methylation of the CpG island of the GSTP1 gene promoter silences GSTP1 gene expression and protein levels, setting the stage for additional genetic damage and accelerated progression toward PIN and carcinoma. Additional results show that AMACR may be an important new marker of prostate cancer, and its use in combination with p63 staining may provide the basis for an improved method for identification of prostate cancer.
"Could Blocking Inflammation Stop Cancer from Forming?" The Holy Grail, for scientists studying evolution, is the idea of a “missing link,” a creature somewhere between man and ape, to explain how humans came to be. Scientists studying prostate cancer are also looking for missing links—more than one, certainly—to explain the complicated journey through which a normal cell evolves into a cancerous one. What lies between Point A and Point B? One step before prostate cancer is PIN, prostatic intraepithelial neoplasia, or “funny-looking” cells that aren’t normal, but aren’t quite cancerous. One likely step before that, as pathologist Angelo De Marzo, M.D. , Ph.D., discovered a couple of years ago, is PIA, proliferative inflammatory atrophy—cells that appear to be shut down, or atrophied, and are surrounded with inflammation. PIA cells, despite their appearance, are actually volatile, with wildly fluctuating levels of glutathione-S -transferase p, which protects against prostate cancer. Is early inflammation of the prostate an important step—even a missing link— to cancer? And is this inflammation a “done deal,” or is it reversible? Oncologists Michael A. Carducci, M.D. , and Theodore DeWeese, M.D. , of the Brady Urological Institute and the Kimmel Cancer Center, interested in the idea of reversing the steps leading to cancer through “chemoprevention,” are hoping to find out. They have started a clinical trial, funded by the National Cancer Institute, of antiinflammatory drugs called COX (cyclooxygenase) inhibitors—a class of drugs that includes NSAIDS (nonsteroidal antiinflammatory drugs) and even plain old aspirin. The particular drug in this trial, a selective COX-2 inhibitor (which has fewer side effects than aspirin and other drugs in this class) called celecoxib, was developed as a treatment for arthritis. “But it turns out,” says Carducci, “that the COX-2 inhibitors also interact heavily with the pathways that are important for cancer progression. The idea, bolstered by research from Angelo De Marzo, Bill Nelson, Ted DeWeese, and others, is that early inflammatory injury—and whether or not the body’s able to repair it—may be the next step to forming cancer. And new evidence suggests that when there’s inflammation, growth factors are produced that promote blood vessel growth, and this also may increase the likelihood that cancer will develop. So it’s becoming increasingly clear that maybe just blocking this pathway could delay disease. ” COX inhibitors are known to lower someone’s risk of developing colon cancer; they also may help prevent esophageal cancer, and some recent studies suggest that men who regularly take aspirin and other COX inhibitors are less likely to develop prostate cancer. “Our research (done in collaboration with Brady molecular geneticist Bill Isaacs) suggests that if these inhibitors do work, they don’t seem to be working by directly affecting the cancer cells themselves,” says De Marzo, “because the target protein of the inhibitor is not present in prostate cancer cells. It’s only present in some of the inflammatory cells, the white blood cells, and in the PIA cells themselves. So it suggests that if these drugs really do inhibit prostate cancer—if these are little fires burning in the prostate—this might put them out.” These early cells, De Marzo notes, are a different kettle of fish altogether from advanced cancer cells. "We want to see whether this is something we should be giving very early in the disease, to someone who’s at high risk, or if taking this could help prevent prostate cancer, like an aspirin a day for your heart.” When we examine a prostate that’s been removed for cancer—even in the ones where there is not a lot of cancer— we see several little, separate cancers,” says De Marzo. “If we could decrease the rate of formation of these little cancers—prevent new lesions from forming—we might stop the big cancers.” In Carducci’s new study, which is “double- blind”—meaning the doctors don’t know who is getting the drug, and who is getting a placebo—men who are scheduled to undergo radical prostatectomy will be given celecoxib for about six weeks, from the time their cancer is diagnosed until the time of surgery. De Marzo, explaining the need to make the study “blind,” quotes Brady scientist Don Coffey, Ph.D. “As Dr. Coffey says, you don’t see with your eyes, you see with your mind, what you expect to see. If you can’t possibly see it, that’s the only way to make it really valid.” “The idea,” says Carducci, “is to look a short-term exposure, and see what the effect of the drug is on inflammation, angiogenesis (growth of new blood vessels to feed the cancer), DNA damage, and cell proliferation. ” After the men undergo surgery, De Marzo will examine the removed prostate tissue. If the COX inhibitor shows promise, the study will be expanded. “We want to see whether this is something we should be giving very early in the disease, to someone who’s at high risk, or if taking this could help prevent prostate cancer, like an aspirin a day for your heart,” says Carducci. De Marzo is conducting longer-term laboratory studies to see whether giving COX inhibitors can prevent prostate cancer in rats. “It would be nice one day,” he envisions, “to give this to younger men, in their 30s and 40s, and say, ‘you don’t have cancer yet, but you have a high risk. Start taking these fairly nontoxic drugs, and they may prevent your prostate cancer, and incidentally, prevent colon cancer. We’re not there yet, but that’s the real potential payoff.” Artikeln är från universitetssjukhuset John Hopkins, Baltimore, USA. http://urology.jhu.edu/news/6/12.html.
Decreased prostatic inflammation using Vitamin D3 Nonn L, Peng L, Feldman D, Peehl DM. Departments of Urology and Medicine, Stanford University School of Medicine, Stanford, California. Inhibition of p38 by Vitamin D Reduces Interleukin-6 Production in Normal Prostate Cells via Mitogen-Activated Protein Kinase Phosphatase 5: Implications for Prostate Cancer Prevention by Vitamin D. Although numerous studies have implicated vitamin D in preventing prostate cancer, the underlying mechanism(s) remains unclear. Using normal human prostatic epithelial cells, we examined the role of mitogen-activated protein kinase phosphatase 5 (MKP5) in mediating cancer preventive activities of vitamin D. Up-regulation of MKP5 mRNA by 1,25-dihydroxyvitamin-D(3) (1,25D) was dependent on the vitamin D receptor. We also identified a putative positive vitamin D response element within the MKP5 promoter that associated with the vitamin D receptor following 1,25D treatment. MKP5 dephosphorylates/inactivates the stress-activated protein kinase p38. Treatment of prostate cells with 1,25D inhibited p38 phosphorylation, and MKP5 small interfering RNA blocked this effect. Activation of p38 and downstream production of interleukin 6 (IL-6) are proinflammatory. Inflammation and IL-6 overexpression have been implicated in the initiation and progression of prostate cancer. 1,25D pretreatment inhibited both UV- and tumor necrosis factor alpha-stimulated IL-6 production in normal cells via p38 inhibition. Consistent with inhibition of p38, 1,25D decreased UV-stimulated IL-6 mRNA stabilization. The ability of 1,25D to up-regulate MKP5 was maintained in primary prostatic adenocarcinoma cells but was absent in metastases-derived prostate cancer cell lines. The inability of 1,25D to regulate MKP5 in the metastasis-derived cancer cells suggests there may be selective pressure to eliminate key tumor suppressor functions of vitamin D during cancer progression. These studies reveal MKP5 as a mediator of p38 inactivation and decreased IL-6 expression by 1,25D in primary prostatic cultures of normal and adenocarcinoma cells, implicating decreased prostatic inflammation as a potential mechanism for prostate cancer prevention by 1,25D. Cancer Res 2006; 66(8): 4516-24).PMID: 16618780 [PubMed - in process] http://cancerres.aacrjournals.org/cgi/content/abstract/66/8/4516
Dr. Roland Wheelers hemsida om ev. samband mellan prostatit och prostacancer Department of Urology, The Prostatitis and Prostate Cancer Center, Sarasota, Florida, USA Dr. Roland Wheelers hemsida finns på följande URL: http://www.peenuts.com/eps.html Där anser han bl.a. (vilket strider mot de flesta andra urologers uppfattning) att det finns ett klart samband mellan kronisk prostatit och prostatacancer? Från hans hemsida citerar jag: "Prostatitis is associated with Prostate cancer. Prostatitits was evident in more than 1100 consecutive patients with Prostate Cancer."
Urology 2003 Feb;61(2):397-401 Leskinen MJ, Vainionp R, Syrjnen S, Leppilahti M, Marttila T, Kylml T, Tammela TL. Department of Urology, Seinajoki Central Hospital, Seinajoki, Finland. To study the possible involvement of viruses in chronic pelvic pain syndrome (CPPS) using polymerase chain reaction. Among other factors, the involvement of viruses in CPPS has been speculated, but few studies have investigated this. Consecutive patients with localized prostate cancer for whom radical prostatectomy was considered were evaluated for symptoms of CPPS using the National Institutes of Health Chronic-Prostatitis Symptom Index. Ten patients with moderate to severe symptoms and 10 without symptoms were included in the study. The presence of herpes simplex virus (types 1 and 2), cytomegalovirus, and human papillomavirus DNA was investigated by polymerase chain reaction in prostatic tissue samples obtained at radical prostatectomy. All the samples were negative for the viral sequences tested. A viral etiology could not be demonstrated in CPPS. In addition, no association of the viruses with prostate cancer could be found.
Prostate, 2003 Apr 7;55(2):105-10 Negative bacterial polymerase chain reaction (PCR) findings in prostate tissue from patients with symptoms of chronic pelvic pain syndrome (CPPS) and localized prostate cancer. Leskinen MJ, Rantakokko-Jalava K, Manninen R, Leppilahti M, Marttila T, Kylmala T, Tammela TL. Department of Urology, Seinajoki Central Hospital, Seinajoki, Finland. BACKGROUND: The etiology of chronic pelvic pain syndrome (CPPS) remains obscure. Although, bacterial etiology has frequently been suggested, evidence of both bacterial involvement in CPPS and the presence of normal bacterial flora in the prostate remain uncertain. MATERIALS AND METHODS: We investigated the presence of bacterial DNA using polymerase chain reaction (PCR) techniques on prostatic tissue samples obtained in radical prostatectomy from 10 patients with moderate to severe symptoms of CPPS and 10 nonsymptomatic patients with localized prostate cancer. For symptom evaluation we used the National Institutes of Health-Chronic Prostatitis Symptom Index (NIH-CPSI). RESULTS: All but one sample were negative for bacterial DNA. The PCR from a symptomatic patient was reproducibly positive in 16S rDNA PCR but negative in 23S rDNA PCR. Bacterial DNA was found in only one out of two sample aliquots and cloning yielded different sequences in two PCR products. CONCLUSIONS: A bacterial etiology for CPPS symptoms could not be demonstrated in patients with prostate cancer. The results also suggest that the prostate is unlikely to harbor bacterial normal flora.
Urology 1999 Mar;53(3):487-91 Keay S, Zhang CO, Baldwin BR, Alexander RB Department of Medicine, University of Maryland School of Medicine, Department of Veterans Affairs Medical Center, Baltimore 21201, USA. OBJECTIVES: A previously reported study using nested polymerase chain reaction (PCR) analysis indicated the presence of DNA from a variety of prokaryotic microorganisms in 77% of transperineal prostate biopsies from patients with chronic nonbacterial prostatitis. Because that study did not include a control group, we investigated whether microbial DNA could also be found in transperineal prostate biopsies obtained from men who did not have a history of prostatitis. METHODS: Transperineal biopsies of both lobes of the prostate were obtained under ultrasound guidance from 9 patients with localized adenocarcinoma of the prostate. DNA was extracted from the prostatic tissue and two- round amplification performed using nested primers from a highly conserved region of the bacterial 16s rRNA gene. Amplified DNA was purified and sequenced, and sequences obtained were compared to bacterial rRNA genes recorded in GenBank. Results. Eleven of 18 biopsy specimens from 8 of 9 patients were positive for bacterial DNA by PCR. Sequence data indicated a predominant organism in 8 of 11 specimens, with greater than 95% homology to DNA from several different genera of bacteria, including Escherichia and Bacteroides. All 9 control samples from the instruments before biopsy were negative. CONCLUSIONS: The presence of bacterial 16s rRNA genes in prostatic tissue is not specific for chronic prostatitis and occurred in most of our patients with localized prostate cancer. Whether the presence of such bacteria is related to the development of prostatic diseases such as prostatitis or prostatic cancer will require carefully controlled trials, including appropriate control groups examined identically.
Prostatitis and Benign Prostate Hyperplasia Often Overlap in Healthy Men NEW YORK (Reuters Health) Mar 11 - Prostatitis is common among healthy US men, and many of these men also report benign prostate hyperplasia (BPH), researchers report in the March issue of the Journal of Urology. "Whether there is a true association or just confusion of symptoms is unknown," they write. Dr. Mary McNaughton Collins from Massachusetts General Hospital, Boston, and associates analyzed data on 31,682 US health professionals, 40 to 75 years of age in 1986, who participated in the Health Professionals Follow-up Study. In 1992 the participants provided information on urological diagnosis, lower urinary tract symptoms and other clinical and lifestyle factors. Sixteen percent of the men reported a history of prostatitis. Among men reporting a history of BPH there was a 7.7-fold increase in the odds of these same men also having a history of prostatitis, the researchers found. They say, "We found it striking that greater than 50% of men with prostatitis reported BPH, and greater than a third with BPH reported prostatitis." Dr. Collins and colleagues identified several correlates of prostatitis, which they suggest may aid in its recognition. Specifically, the investigators found that men reporting moderate lower urinary tract symptoms had a 1.8-fold increased odds of having prostatitis and men with severe lower urinary tract symptoms had a 2.8-fold higher odds for prostatitis. Prostatitis was also associated with a history of sexually transmitted disease (1.8-fold greater odds), and stress at home (1.5-fold greater odds) and work (1.2-fold greater odds), Dr. Collins's team reports. J Urology 2002;167:1363-1366.
THE JOURNAL OF UROLOGY 2002;167:2267-2270 Robert E. Gerstenbluth; Allen D. Seftel*; Gregory T. MacLennan; R. Nagarjun Rao; Eric W. Corty?; Kelly Ferguson; Martin I. Resnick? From the Departments of Urology and Pathology, Case Western Reserve University, University Hospitals of Cleveland, Cleveland Veterans Affairs Medical Center, Cleveland, Ohio, and Pennsylvania State University, Behrend College, Erie, Pennsylania. Purpose: We examined the anatomical relationship of chronic prostatitis with prostate cancer and benign prostatic hyperplasia (BPH) based on the hypothesis that there may be an association of prostatitis with these other entities that may involve up-regulation of bcl-2. Materials and Methods: We examined 40 whole mount radical prostatectomy specimens for the presence and distribution of chronic inflammatory infiltrate. Immunostaining for bcl-2 was done in 10 cases. Results: Chronic prostatitis was identified in all 40 cases with peripheral zone inflammation in 95% and transition zone inflammation in 87.5%. In all cases of transition zone inflammation the infiltrate was noted within and/or around BPH. Inflammatory infiltrate was microscopically associated with prostate cancer in 23 of the 40 cases (57.5%). In these 23 cases, there was no association of inflammation with Gleason score, preoperative prostate specific antigen, positive margins, or seminal vesicle invasion. Patients with BPH unassociated with prostatitis had significantly smaller prostate weight (median 32 gm.) and were younger (mean age 54.4 years) than those with BPH associated with prostatitis (median weight 40 gm. and mean age 61.4 years, p <0.05). Bcl-2 staining was intensified in benign glands within areas of prostatitis in all 10 cases examined. Conclusions: Chronic prostatitis is a common finding in radical prostatectomy specimens. Inflammation was associated with BPH and cancer but had a greater tendency to be associated with BPH. Bcl-2 was prominently expressed in areas of prostatitis. Our findings indirectly support a potential role for prostatitis in the pathogenesis of BPH.
Virus som orsak till prostatacancer Från den 31 mars 2006. Forskare i USA har hittat ett hitills okänt virus XMRV i tumörvävnad hos män med prostatacancer. Det är nära besläktat med ett annat virus som kan ge upphov till leukemi hos möss. I Public Library of Science skriver forskarna att man tror att viruset smittar mellan människor. Upptäckten innebär att man för första gången kan börja leta efter ett samband mellan virusinfektion och prostatacancer. Det här är ett forskningsgenombrott säger Jan-Erik Damber, Professor i urologi vid Sahlgrenska Universitetssjukhuset. Vid t.ex. livmoderhals- och levercancer vet man redan att virus har betydelse för uppkomsten, men detta har inte tidigare kunnat fastslås vid prostatacancer. XMRV hittades bara hos män med en speciell genuppsättning.
Endocrine patterns in patients with benign and malignant prostatic diseases Prostate 2000 Aug 1;44(3):219-24 Related Articles, Books, LinkOut Schatzl G, Reiter WJ, Thurridl T, Waldmuller J, Roden M, Soregi S, Madersbacher S. Department of Urology, University of Vienna, Vienna, Austria. BACKGROUND: The known importance of the endocrine system, particularly of steroid hormones, for development of the prostate gland and the fact that steroid hormones act as immunmodulators prompted us to compare hypophyseal, adrenal, and gonadal hormones, including cortisol, in patients with benign and malignant prostatic diseases. METHODS: Patients with newly diagnosed, untreated prostate cancer (PC) (n = 75) and, as a control population, those with untreated lower urinary tract symptoms (LUTS) due to benign prostatic hyperplasia (BPH) (n = 159) entered this prospective study. In all patients, the following parameters were obtained by serum analysis: prostate-specific antigen (PSA), human luteinizing hormone (hLH), human follicle-stimulating hormone (hFSH), testosterone, estradiol (E2), cortisol, and dehydroepiandrosterone-sulphate (DHEA-S). Serum samples were collected of fasting patiens between 7. 30-10.00 AM. RESULTS: Age was comparable in both groups (PC: 65.6 +/- 7.6 years (mean +/- standard deviation) vs. controls:64.9 +/- 8. 1 years; P = 0.56). HFSH (PC: 6.6 +/- 3.9 mIU/ml; controls: 8.4 +/- 6.4 mIU/ml; P = 0.04), hLH (PC: 5.3 +/- 4.8mIU/ml; controls: 7.6 +/- 6.2 mIU/ml; P = 0.009), and estradiol (PC: 25.8 +/- 12.7 pg/ml; controls: 32.6 +/- 12.6 pg/ml; P = 0.0003) were significantly lower in PC patients than controls. Cortisol (PC: 16.7 +/- 4.2 microg/dl; controls: 13.5 +/- 4.3 microg/dl; P < 0.0001) was significantly higher in cases. The difference for cortisol and estradiol concentrations between PC patients and controls held true in all life-decades. Serum concentrations for DHEA-S and testosterone were comparable between PC and control patients. In PC patients, none of the endocrine parameters correlated to serum PSA or clinical/pathological stage. CONCLUSIONS: Patients with newly diagnosed, untreated PC yielded significantly higher cortisol and lower estradiol serum concentrations than controls. The known effect of cortisol on the immune status warrants further studies.
JAMA, January 3, 2001;285:47-51. 1 Serotypes of Chlamydia trachomatis and Risk for Development of Cervical Squamous Cell Carcinoma Aini Bloigu, BSc Joakim Dillner, MD Irma Ika¨ heimo, PhD Egil Jellum, PhD Matti Lehtinen, MD Per Lenner, MD Timo Hakulinen, PhD Ale Na¨ rva¨ nen, PhD Eero Pukkala, PhD Steinar Thoresen, MD Linda Youngman, PhD Jorma Paavonen, MD Objective: To study the association between exposure to different C trachomatis serotypes and subsequent development of cervical SCC. Design and Setting: Longitudinal, nested casecontrol study within a cohort of 530 000 women who provided samples to serum banks in Finland, Norway, and Sweden. The data files were linked to respective national cancer registries. Subjects: One hundred twentyeight women who had developed invasive cervical SCC at least 12 months following serum donation. Each case had 3 matched controls. Main Outcome: Measure Risk for the development of cervical SCC by IgG antibodies to 10 different C trachomatis serotypes, adjusted for antibodies to HPV types 16, 18, and 33 and for serum cotinine levels. Results Of specific C trachomatis serotypes, serotype G was most strongly associated with SCC (adjusted odds ratio [OR], 6.6; 95% confidence interval [CI], 1.6-27.0). Other serotypes associated with SCC were I (OR, 3.8; 95% CI, 1.3-11.0) and D (OR, 2.7; 95% CI, 1.3-5.6). Presence of serum IgG antibodies to more than 1 serotype increased the adjusted ORs for SCC (P,.001 for trend). Conclusions: Chlamydia trachomatis serotype G is most strongly associated with subsequent development of cervical SCC. Increasing numbers of exposures to different C trachomatis serotypes also increases risk. Our results strengthen the evidence that there is a link between past C trachomatis infection and cervical SCC.
JAMA, January 3, 2001;285:47-51. 2 EDITORIAL Chlamydia and Cervical Cancer A Real Association? Jonathan M. Zenilman, MD WORLDWIDE, CERVICAL CANCER IS AMONG THE 3 most prevalent malignancies in women, with more than 400000 cases reported in 1998, of which 12800 were in the United States.1 The causal relationship between subtypes of human papillomavirus (HPV) and cervical cancer has been firmly established.. The epidemiological data are compelling and consistent, most recently from nested casecontrol studies in Scandinavia that demonstrated HPV in specimens collected before incident cervical intraepithelial neoplasia (CIN).2,3 However, there are still important unanswered questions related to pathogenesis. Human papillomavirus infection is common. In adolescent populations, infection rates as high as 44% to 90% have been observed.4-6 Recent data strongly suggest that the majority of persons with HPV spontaneously clear the infection without any specific medical intervention. Only a small minority of these infected persons develop cervical dysplasia, and of these, a minority develop invasive carcinomas. Therefore, the involvement of cofactors in the pathogenesis of HPV-related complications has been suspected. From a methodological standpoint, identifying cofactors for cervical cancer is difficult. As a sexually transmitted infection (STI), HPV has numerous potential behavioral and clinical confounders. For example, sexual behavior variables such as number of partners also are related to infection with other STIs. Since the progression from HPV infection to CIN takes years, cofactors could be operative at different points in the natural history of HPV infection, either during incident infection, having an impact on potential clearance, or during the prolonged period of latent infection. Study designs that can tease out these numerous variables are critical. Because of the relatively low incidence of cervical carcinoma, large populations are required to sort out these issues. Smoking, to which people are typically exposed long term, has been consistently identified as a risk for progression of HPV infection to CIN.5-8 In serological studies, smoking at the time of serum collection can be validated by measurement of cotinine levels. The literature on the causes of cervical cancer is replete with classic tales of epidemiologic confounders. Before the discovery of HPV, carefully performed studies attempted to link cervical cancer with STIs. In 1970, Nahmias et al 9 demonstrated in a casecontrol study of Atlanta maternity patients that herpes simplex virus 2 was associated with cervical cancer. Schachter et al 10 similarly attempted to determine the association between Chlamydia trachomatis infection and cervical cancer. These studies did not control for sexual behavior, nor did they account for the yet undiscovered HPV, and are in retrospect inconclusive. Later associations of cervical cancer with C trachomatis were identified in several of the initial investigations that linked HPV to cervical carcinoma. In an STI clinic study conducted between 1984 and 1986, Koutsky et al 11 evaluated the association of CIN with HPV. After adjustment for HPV status, CIN was also associated independently with serological evidence of either infection with chlamydia, gonorrhea, or cy-tomegalovirus. Lehtinen et al 12 used data from a Finnish national mobile health examination survey conducted between 1966 and 1972 to link results with subsequent cervical cancers reported to the national registry. They found that prior chlamydial infection was significantly associated with cervical carcinoma, with higher levels of significance for serotype pool GFK, but the study was limited by small numbers of cancers and the lack of multivariate analysis. In contrast, crosssectional studies in southwestern US populations 13 and a series of casecontrol studies in Honduras,14 Colombia, and Spain 15 failed to demonstrate an association between chlamydial infection (or any other STI) and cervical cancer. The study by Anttila and colleagues 16 in this issue of THE JOURNAL is 1 of a series of investigations that have used data from large serum banks (in this case, collected from more than 530000 individuals in 3 Nordic countries) and matched these data with subsequent cervical cancer cases collected by national cancer registries.17 Since the baseline specimens were collected an average of 56 months before the cytological diagnosis of cervical cancer, the causal inference is substantial.The Nordic studies strongly suggest that there is an independent relationship between C trachomatis infection and cervical squamous cell carcinoma (SCC), after controlling for HPV infection and smoking. In the study by Anttila et al, multiple tests for C trachomatis serology were used with an emphasis on specificity. Highest point estimates involved longer lag times between donating the serum and developing cervical cancer. The authors note that specific serotypes (G, I, and D) were more likely to be associated with SCC than the others. These data, as the authors acknowledge, parallel a previous report from Finland that suggests that the serotype pool GFK is associated with the development of CIN.12 However, the findings of Anttila et al, while provocative, are lim-ited by the small sample sizes used for these estimates and by the consequent wide confidence limits (as demonstrated in Table 1 of their article). Confirmation of this finding is therefore important. Anttila et al also report that C trachomatis DNA was found in 5% of the cases of CIN. Since C trachomatis causes a curable bacterial infection, DNA is not likely to be present in situations where the infection has already been treated. Also, the DNA may represent new, recent chlamydial infections (ie, those occurring after malignant transformation had already occurred). Despite its elegant nested casecontrol design, the study has limitations. There are limited behavioral data associated with either the baseline serum measurement or the subsequent CIN diagnosis. Therefore, the possibility of an additional unmeasured behavioral or biological confounder cannot be excluded. Nevertheless, the results lead to a number of intriguing questions. How does C trachomatis enhance the progression of HPV to invasive cervical cancer? Since HPV viral load has been associated with subsequent development of CIN,18 does bacterial infection, or the consequent mucosal inflammation, induce a transactivationlike response resulting in an increased viral load? Does chlamydial infection or other STI modify the host inflammatory or immunological response to HPV? Do these infections modify the spontaneous clearance rate of HPV? Chlamydia can present as an acute infection or as one that is asymptomatic and persistent. Is the cancerpromoter effect related to duration of infection? Is chlamydia an independent risk factor? The data also provide potential clinical relevance to the chlamydia typing system. The chlamydia serotypes have been used mostly as epidemiologic research tools. Specific serotypes have been linked to clinical syndromes: serotype D with pelvic inflammatory disease,19 serotypes F and G with symptomatic rectal infection,20 serotype F with asymptomatic cervical infection, 21 and more recently, serotype C with persistent cervical infection.22 All of these studies, however, had small sample sizes and the results are therefore not generalizable. Until recently, the accumulation of these serotype data would have been little more than a curiosity to nonepidemiologists. If the results of Anttila and colleagues (that serotypes D, G, and I are related to increased rates of CIN) are confirmed, a series of public health responses could follow. The obvious research question to evaluate is what outer membrane protein components are involved in the potential promoter effect. The sequencing of the chlamydia genome 23 facilitates further research into determining the membrane and genetic correlates of these findings, all of which should allow more insight into the pathogenesis of chlamydia and its complications. Moreover, the findings of Anttila et al suggest that cervical malignancy should be added to the complications and costs associated with genital chlamydial infections. These complications include pelvic inflammatory disease, infertility, and facilitated transmission of human immunodeficiency virus. These data provide additional justification for expanding chlamydial infection screening, not only to protect against pelvic inflammatory disease and infertility, but potentially to prevent cervical cancer. Acknowledgment: I thank Keerti Shah, MD, and Thomas Quinn, MD, for their helpful comments. REFERENCES 1. National Cancer Institute. Cervical cancer: backgrounder. Available at: http://rex.nci.nih.gov/massmedia/backgrounders/cervical.html. Access verified De-cember 1, 2000. 2. Reeves WC, Brinton LA, Garcia M, et al. Human papillomavirus infection and cervical cancer in Latin America. N Engl J Med. 1989;320:1437-1441. 3. Wallin KL, Wiklund F, Angstrom T, et al. Type-specific persistence of human papillomavirus DNA before the development of invasive cervical cancer. N Engl J Med. 1999;341:1633-1638. 4. Jacobson DL, Womack SD, Peralta L, et al. Concordance of human papilloma-virus in the cervix and urine among inner city adolescents. Pediatr Infect Dis J. 2000;19:722-728. 5. Bauer HM, Hildesheim A, Schiffman MH, et al. Determinants of genital human papillomavirus infection in low-risk women in Portland, Oregon. Sex Transm Dis. 1993;20:274-278. 6. Bauer HM, Ting Y, Greer CE, et al. Genital human papillomavirus infection in female university students as determined by a PCR-based method. JAMA. 1991; 265:472-477. 7. La Vecchia C, Franceschi S, Decarli A, Fasoli M, Gentile A, Tognoni G. Cigarette smoking and the risk of cervical neoplasia. Am J Epidemiol. 1986;123:22-29. 8. Nischan P, Ebeling K, Schindler C. Smoking and invasive cervical cancer risk: results from a case-control study. Am J Epidemiol. 1988;128:74-77. 9. Nahmias AJ, Josey WE, Naib ZM, Luce CF, Guest BA. Antibodies to Herpesvi-rus hominis types 1 and 2 in humans, II: women with cervical cancer. Am J Epi-demiol. 1970;91:547-552. 10. Schachter J, Hill EC, King EB, et al. Chlamydia trachomatis and cervical neo-plasia. JAMA. 1982;248:2134-2138. 11. Koutsky LA, Holmes KK, Critchlow CW, et al. A cohort study of the risk of cervical intraepithelial neoplasia grade 2 or 3 in relation to papillomavirus infec-tion. N Engl J Med. 1992;327:1272-1278. 12. Lehtinen M, Dillner J, Knekt P, et al. Serologically diagnosed infection with human papillomavirus type 16 and risk for subsequent development of cervical carcinoma: nested case-control study. BMJ. 1996;312:537-539. 13. Becker TM, Wheeler CM, McGough NS, et al. Sexually transmitted diseases and other risk factors for cervical dysplasia among southwestern Hispanic and non-Hispanic white women. JAMA. 1994;271:1181-1188. 14. Ferrera A, Baay MF, Herbrink P, Figueroa M, Velema JP, Melchers WJ. A sero-epidemiological study of the relationship between sexually transmitted agents and cervical cancer in Honduras. Int J Cancer. 1997;73:781-785. 15. de Sanjose S, Munoz N, Bosch FX, et al. Sexually transmitted agents and cervicalneoplasia in Colombia and Spain. Int J Cancer. 1994;56:358-363. 16. Anttila T, Saikku P, Koskela P, et al. Serotypes of Chlamydia trachomatis and risk for development of cervical squamous cell carcinoma. JAMA.2001;285:47-51. 17. Koskela P, Anttila T, Bjorge T, et al. Chlamydia trachomatis infection as a risk factor for invasive cervical cancer. Int J Cancer. 2000;85:35-39. 18. Ylitalo N, Sorensen P, Josefsson AM, et al. Consistent high viral load of hu-?
Är en "klackspark" svenska sjukvårdsansvarigas syn på ovanstående?
Tillbaka till Appell till den svenska sjukvården
Tillbaka till Blandat innehåll
Tillbaka till Brevkontakt med Cancerfonden
Tillbaka till Orsak (på sidan Prostatasjukdomarna)
|