|
— information som av olika anledningar är av speciellt intresse —
Här finns bl.a. uppgifter om olika Workshop och information som av olika anledningar är av ett speciellt intresse. De korta notiserna i slutet på sidan täcker olika aspekter på kronisk prostatit och interstitiell cystit och väl värda en genomläsning.
Inlagt 2007-09-14. Enligt underhandsuppgifter har Kärnsjukhuset i Skövde som första svenska sjukhus på försök startat upp en "speciell mottagning" för män med kronisk prostatit. Detta för att kunna ge stöd, kontinuitet och pröva nya behandlingsupplägg. Vi kan bara hoppas att andra Landsting/sjukhus uppmärksammar detta, tar sitt ansvar och inser att det finns ett stort behov av en sådan mottagning.
The Multidisciplinary Approach to Chronic Pelvic Pain Syndromes, Workshop 2008 URL: http://www3.niddk.nih.gov/fund/other/UrologicPainSynd/index.htm International Symposium on definitions: Date for your diary! The National Institutes of Health /National Institute of Diabetes & Digestive & Kidney Diseases (NIH/NIDDK) have announced that an International Symposium will be held in Bethesda, Maryland, USA, 16-17 June 2008, entitled: Defining the Urologic Chronic Pelvic Pain Syndromes – A New Beginning. This will be your chance to participate and have your say on this important issue, so put this date in your diary now!
NIH/NIDDK Workshop on “The Multidisciplinary Approach to Defining the Urologic Chronic Pelvic Pain Syndromes” held in Baltimore, 13/14 DecemberThe over forty participants attending this brainstorming workshop in Baltimore included doctors from the USA, Canada, Europe, Japan, India and Taiwan from various medical disciplines, representatives from industry, as well as a number of representatives from the patient movement including the IPBF. The overall purpose of the Urologic Chronic Pelvic Pain Working Group is to redefine the two major urologic pelvic pain syndromes (Interstitial Cystitis/Painful Bladder Syndrome and Chronic Prostatitis/Chronic Pelvic Pain Syndrome) in the context of the other major syndromes with which they are commonly associated (Chronic Fatigue Syndrome, Fibromyalgia, Irritable Bowel Syndrome, Vulvodynia and others). The definitions will be finalized at the Symposium in June 2008. These definitions will be utilized for research studies so that published data in all of these relevant areas will be using a common working definition. The main aims of this workshop were to discuss the disease definitions and diagnostic protocols of the major Chronic Pelvic Pain Co-Morbid Disorders (Interstitial Cystitis, Chronic Prostatitis, Fibromyalgia, Chronic Fatigue Syndrome and Irritable Bowel Syndrome); to discuss interrelationships among these disorders; to identify common symptomatology; to discuss methodology for a comprehensive diagnostic evaluation of persons with these symptoms to ensure a complete evaluation for all relevant co-morbidities. In other words, this workshop aimed to set in motion a new approach to PBS/IC and CP/CPPS, based on relationships with other pain syndromes, and to look for a common pathway and links between the syndromes. It was specifically not the intention of this workshop to discuss names.- Day one included presentations on evidence for an interrelationship between the chronic pelvic pain disorders covering fibromyalgia, chronic fatigue syndrome, irritable bowel syndrome, vulvodynia, chronic abacterial prostatitis/CPPS and IC/PBS and what symptoms all these conditions have in common and to what extent they overlap. - Day two was used to summarise the previous day’s intensive discussions. The intention is for two articles to be published: one outlining why the disorders are thought to be related and a second explaining how this changes the way we look at urologic pain syndromes. - Rounding off the workshop, it was concluded that while the perspective has become broader in terms of how the disorder is going to be viewed, IC and CP will not lose their unique identity. Dr Leroy Nyberg from the NIDDK explained that IC and CP have now become part of a large family with many different cousins. Rheumatologist Professor Daniel Clauw (USA) and urologist Professor Jorgen Nordling (Denmark) also reminded us that we should not forget that there may be groups of PBS/IC patients who only have a bladder problem and not a systemic disorder. It is hoped that future studies will identify these groups. In the meantime a special NIDDK website will be set up on which a summary of this workshop will be placed along with all new developments in the coming period. We will let you know as soon as this website has been launched. It will hopefully be in January 2008. URL: http://www3.niddk.nih.gov/fund/other/UrologicPainSynd/index.htm
NIH Seeks New Research for Prostatitis/CPPS, USA September 21, 2007 The RFA, Multi-disciplinary Approach to the Study of Chronic Pelvic Pain (MAPP) Research Network (RFA-DK-07-003) is now published on the NIH website http://grants.nih.gov/grants/guide/rfa-files/RFA-DK-07-003.html.
The NIDDK funding commitment for this program is up to $7.5 million per year for a five year funding period. We expect to fund up to six Discovery Sites at $1,000,000 Total Costs each year, as well as a separately funded Data Coordinating/Administrative Core and a Tissue Analysis and Technology Core (each to be supported at $750,000 in Total Costs per year). This unique program promotes basic, translational, and clinical science interactions and multi-disciplinary, collaborative approaches using varied expertise from the urology field and from investigators not traditionally involved in chronic urologic pain research to address unmet needs in our understanding of IC/PBS and CP/CPPS. We are encouraging investigators to build strong multi-disciplinary teams to address the goals of this effort and to submit applications for this new and important NIDDK solicitation. Note: The receipt date for applications is January 9, 2008. All inquiries should be directed (preferably by Email) to either Dr. Chris Mullins (MullinsC@extra.niddk.nih.gov) or Dr. Lee Nyberg (NybergL@mail.nih.gov). Also, we have established a website for the program (see RFA text) that we will be populating with pertinent information and the NIDDK will host an in-person information session in Bethesda on November 5th, 2007.
New research definitions/diagnostic protocols of the Urologic CPPS, USA September 2007. The following information concerns upcoming workshops which will explore the interrelationship of the chronic pelvic pain disorders and redefine them in light of published information. The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) of the National Institutes of Health (NIH) has had a long standing commitment to funding research studies and programmes designed to provide insight into the two major urologic pelvic pain syndromes: Interstitial Cystitis/Painful Bladder Syndrome (IC/PBS) and Chronic Prostatitis/Chronic Pelvic Pain Syndrome (CP/CPPS). A major outcome of these endeavours has been that many significant journal articles have been published focusing on these two disorders, independent investigation worldwide has been stimulated and clinicians are much more aware of the existence and significance of these disorders. Despite these significant accomplishments, there has been little progress made in understanding the etiology, pathophysiology, or effective treatment or prevention of these disorders.
On December 13th and 14th a draft of new research definitions/diagnostic protocols of the Urologic CPPS, defined in relation to their co-morbid disorders, and developed using existing published literature, will be finalized by an international panel of clinician experts. These clinicians will then “field-test” the definitions/protocols at their clinics. There will be an opportunity to comment by Email on the proposed definitions, prior to the December meeting. All of these Email comments will be presented to the expert panel. A symposium will then be held in 2008 to evaluate the field testing results and to adjust the draft definition/diagnostic protocol to the pertinent findings of these studies. At this meeting, an open forum will also be held for comments from all interested parties. The definitions developed at the 2008 meeting will then be published and used for future NIDDK funded clinical studies. It is realized that the definitions finalized in 2008 will be based on the current published literature which leaves many relevant questions unanswered. As more peer-reviewed data is published, the definitions will be reviewed and adjusted, if necessary, to ensure the definitions reflect the most recent published data. The December 2007 meeting will be an intense working meeting of clinical specialists from diverse clinical areas, space is very limited and advance registration will be required for admission. Registration will be limited to one person from an organization and will be closed when the limited seating capacity is met. Contact: For further information related to the December CPPS definitions meeting and to be placed on the pre-registration information list, and/or the Email comment list, contact Ms. Cerena Cantrell, The Scientific Consulting Group, Email: ccantrell@scgcorp.com
Jag är tacksam för alla bidrag som passar in under denna rubrik A more detailed list of conferences with contact addresses and websites can be found on our website under "Calendar". - P.U.R.E. H.O.P.E. 4th Annual Pelvic Health Conference Saturday 24 January 2009, Houston, Texas, USA - WIP2009 5th World Congress World Institute of Pain 13-16 March 2009, New York, NY, USA - 24th European Association of Urology (EAU) Congress 17-21 March 2009. Stockholm, Sweden - American Urological Association (AUA) annual conference 25-30 April 2009, Chicago USA - ESSIC Annual Meeting 4-6 June 2009, Göteborg, Sweden - World Continence Week 22-28 June 2009 -
39th Annual Meeting of the International Continence Society – ICS San
Francisco, - 10th International Symposium on Sjogren's Syndrome 1-3 October, 2009, Brest, France. - 30th Congress of the Societe Internationale d’Urologie (SIU) 1-5 November 2009, Shanghai, Chin
Official Webcasts from the SIU (Société Internationale d'Urologie) Meeting 2005, Argentina I en Webcast kan man följa föreläsningen och se de bilder som presenteras som om man "vore på plats". Bredband är bäst, men vanligt modem går oftast också bra även om talet och bilderna kan bli något hackiga. Nerladdningen tar givetvis längre tid. Official Webcasts from the SIU (Société Internationale d'Urologie) Meeting on Prostatic disease Bariloche, Argentina. Sept. 29-Oct. 1, 2005. http://webcasts.prous.com/SIU2005/. Observera i första hand föreläsningarna: -
Chronic Prostatitis/Chronic Pelvic Pain Syndrome: An Evidence-Based Treatment
Strategy. Dr. J. Curtis Nickel, - Acute and Chronic Bacterial Prostatitis: A Practical Diagnosis and Treatment Strategy. Dr. Daniel Shoskes, USA. - Prostatitis. Dr. Bernard Lobel, France. Vi kan i ovanstående Webcast följa föreläsningar av några av världens ledande forskare inom området kronisk prostatit/CPPS.
The American Urological Association (AUA)'s Annual Meeting is the largest meeting of urologic professionals in the world. With more than 10,000 urologists and health-care professionals and 5,000 exhibitors in attendance, there is no better place to learn about the latest advances in urology. Mötesplats 2006: Den 20-25 maj i Atlanta, Georgia,USA. Huvudsida http://www.aua2006.org/am06/ De abstracts som presenterades om prostatit nås genom att klicka på Abstracts och följ sedan anvisningarna. På
http://webcasts.prous.com/Aua2006/article.asp?AID=30&CID=YY&CLID=2
finns en förteckning över Webcasts från årets möte. Bl.a. finns en föreläsning
om prostatit och en om samband mellan inflammation (kronisk prostatit) och
en ev. senare utveckling av prostatcancer. Under Webcast Program klicka
på aktuellt anförande och därefter på Proceed
to Webcast och
välj den internetanslutning som är aktuell.
En information gjord av Interstitial Cystitis Association från AUA IC plenary session 2005 finns på följande: http://www.ichelp.org/FeatureArticles/AUAAMICPlenarySession.html och http://www.ichelp.org/FeatureArticles/ICNewsFrom2005AUAAnnualMeeting.html Se även The Prostatitis Foundations hemsida: http://www.prostatitis.org/AmericanUrologicalMeeting06.html
NIH (National Institutes of Health, USA), Prostatitis/CPPS Workshop 2005
After
years of research and speculation, we still have no clear etiology or
pathogenesis for chronic pelvic pain syndrome/chronic prostatitis (CPPS/CP).
Tillbaka till Personligt från Webmaster
European Association of Urology Meeting Istanbul 2005 Abstracts från detta möte rörande kronisk prostatit/CPPS finns på http://www.urotoday.org/prod/contents/confreport/article.asp?cat=confReport&sid=184&tid=397&aid=2415
Institute of Medicine Forum on Emerging Infections: Linking Infectious Agents and Chronic Diseases Siobhán O’Connor,* Thomas M. Shinnick,* and Christopher E. Taylor *Centers for Disease Control and Prevention, Atlanta, Georgia, USA; and National Institutes of Health, Bethesda, Maryland, USA Siobhán O’Connor, Centers for Disease Control and Prevention, 1600 Clifton Rd., NE, MS C12, Atlanta, GA 30333, USA; fax: 404-639-3039; e-mail: sbo5@cdc.gov Ovanstående författare har sammanställt ett intressant materiel om eventuella samband mellan infektioner och kroniska sjukdomar. Finns på http://www.cdc.gov/ncidod/EID/vol8no12/02-0717.htm
Microbiology Department, Louis Mourier University Hospital, Colombes, France. Email: marie-laure.joly-guillou@lmr.ap-hop-paris.fr Bacterial infections of the male genital tract in young men (<35 years old) are primarily caused by sexually transmissible bacteria like Chlamydia trachomatis, Neisseria gonorrhoeae but also Mycoplasma or Haemophilus spp. In men aged over 35 years, Enterobacteriaceae are more frequently involved in urethritis, epididymitis and prostatitis. The traditional treatments suggested like tetracyclines or erythromycin are less effective since bacterial resistance is increasingly frequent, particularly in N. gonorrhoeae. Moreover, patient compliance with these drug treatments are frequently not well observed. New therapies including short term therapy with fluoroquinolones or azalides (e.g. azithromycin) are very effective and easy to use and thus eliminate any problem of compliance. However, we have to be vigilant for the emergence of resistant strains to these agents
Enligt en artikel i Parade Magazine June 20, 2004 av Dr. Isadore Rosenfeld http://archive.parade.com/index.html finns en ökad risk för akut prostatit om du samtidigt har nedanstående. Akut prostatit (en bakteriell infektion) innebär oftast omedelbart behov av läkarvård (risk för blodförgiftning, sepsis) eftersom symtomen vanligtvis är hög feber, svåra smärtor, urineringsbesvär, frossa och ett kraftigt försämrat allmäntillstånd. You’re most likely to get acute bacterial prostatitis - the most severe form, though treatable - if you have:
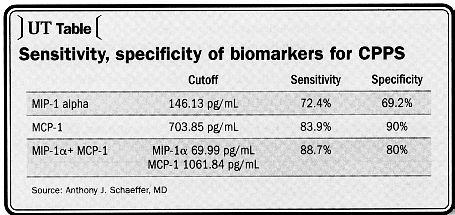
Dr. Anthony J. Schaeffer, MD. Northwestern School of Medicine, Chicago. Reprint from Urology Times, August 15, 2005. A study from Dr. Schaeffer's own lab identified two new biomarkers in expressed prostatic secretions that appear not only to have a high degree of sensitivity and specificity for CPPS, but may also shed light on the pathogenesis of the disease. The cytokine macrophage inflammatory protein-lalpha (MIP-1α has a sensitivity of 72.4% and a specificity of 69.2%; monocyte chemoattractant protein-1 (MCP-1) has a sensitivity of 83.9% and a specificity of 90%. Combined, the two have a sensitivity of 88.7% and a sensitivity of 80%. "Men with CCPS frequently have prostatic inflammation. This study indicates that they also have these two elevated cytokines. These may, in fact, be biomarkers for the disease. Further study is needed to determine how these biomarkers are modulated during the course of the disease and if treatment with anti-cytokines might be warranted," Dr. Schaeffer said.
Företckning
över över studier som berör prostatit (prostatitis) och som administreras av
the U.S. National Institutes of Health http://clinicaltrials.gov/ct/search;jsessionid=8083096910C2A1352984C89D9EB148A8?term=
En sammanställning över deras forskning inom hela urologiområdet finns på http://www.prostate-research.org.uk/research/research.htm
Pressrelease 2007-02-22 Prostavac® is the world's first patented immune-therapeutic vaccine for the treatment of Benign Prostatic Hyperplasia (BPH) and acute/chronic Prostatitis. It has shown a high success rate with 75 per cent of patients showing sustainable improvements, with marginal side effects and no surgery. Due to these factors, it has the potential to become an industry standard. Mer
information finns på följande hemsida: http://www.redorbit.com/news/health/849882/frost__sullivan_enabling_technology_of_the_year_award_2006 Hemsida hos det Schweiziska läkemedelsföretaget AmVac AG som har utvecklat produkten är http://www.amvac.ch
Daily
Mail
11 March 2007, Health. The impotence drug Viagra could help men suffering from pelvic pain. As many as one in ten men in the UK have pelvic pain syndrome, with symptoms including lower back and groin pain, and bladder problems. A trial has been looking at the use of the drug - originally developed to help angina patients, but now widely used to treat impotence - to see if it can help to open the constricted blood vessels that may be the source of the discomfort. Pelvic pain syndrome is the most common urological problem diagnosed in men under 50, and affects up to 10per cent of men in the UK. A report from the Cleveland Clinic in America says 50 per cent of men will experience symptoms during their life. A report in the British Medical Journal described the impact of the disease on the lives of patients with the severest symptoms as comparable to that of men with heart disease. An earlier study by other researchers, of men with erectile dysfunction problems, showed that as well as improved sexual function, they experienced a reduction in other pelvic syndrome symptoms when treated with Viagra. Hela artikeln finns på Daily Mails hemsida:
Kronisk prostatit - ingen evidens för någonting Läkartidningen - Volym 97 - Nr 50 - 2000 URL: http://www.lakartidningen.se Det finns idag inget diagnostiskt test som kan betraktas som "gold standard" för kronisk prostatit och de diagnostiska studier som finns håller låg kvalitet. De få kontrollerade behandlingsstudierna är metodologiskt svaga och studiegrupperna är små. Det finns idag ingen evidens för vare sig antibiotikabehandling eller behandling med a-blockerare. Detta är slutsatserna i en strukturerad analys av den tillgängliga litteraturen om diagnostik och behandling av kronisk prostatit (1). Författarna hade sökt efter kontrollerade diagnostiska studier och randomiserade, kontrollerade behandlingsstudier i MEDLINE, Cochrane library och i bibliografier i relevanta artiklar. Man fann 19 diagnostiska studier och 14 behandlingsstudier som uppfyllde kriterierna. De diagnostiska artiklarna rörde diagnos av infektion och inflammation, immunologi, biokemi, ultraljud och psykologiska test. Inte någon att dessa diagnostiska principer kunde säkert användas för diagnosen kronisk prostatit. Behandlingsartiklarna rörde a-blockerare, finasterid, antiinflammatoriska medel, antibiotika, värmebehandling och andra varierande medikamenter. Det fanns inget vetenskapligt stöd för att någon av dessa behandlingar hade en gynnsam effekt för patienten. Således är kunskapen om kronisk prostatit minst sagt dålig. En grundorsak till detta är säkerligen att diagnosen som sådan är odefinierad och oklar. Två steg på vägen till bättring är troligen den nya klassifikation av prostatit som föreslagits av National Institute of Diabetes and Digestive and Kidney Diseases (NIDDIK) (2) och det nya symtomformulär som tagits fram av National Institutes of Health (3). Även om dessa instrument ännu inte är helt optimala så är de användbara verktyg för att börja nysta upp diagnosen kronisk prostatit. 1. Ann Intern Med 2000; 133: 367-81. 2. JAMA 1999; 282: 236-37. 3. J Urol 1999; 162: 369-75. Jan Adolfsson SBU, Statens Beredning för medicinsk Utvärdering, Tyrgatan 7, Box 5650, 114 86 Stockholm. Tfn: 08-412 32 00 http://www.sbu.se
The aetiology of chronic prostatitis is not understood Clin Exp Immunol 2002 May;128(2):302-7 Batstone GR, Doble A, Gaston JS. Department of Urology, Addenbrooke's Hospital, Cambridge, UK. grd@batstoner.fsnet.co.uk The aetiology of chronic prostatitis is not understood. The aim of this study is to investigate an autoimmune hypothesis by looking for T cell proliferation in response to proteins of the seminal plasma. We studied peripheral blood mononuclear cell proliferation from 20 patients with chronic prostatitis and 20 aged-matched controls in response to serial dilutions of seminal plasma (SP) from themselves (autologous SP) and from a healthy individual without the disease (allo-SP). We found that the patients have a statistically greater lymphocyte proliferation to autologous SP at the 1/50 dilution on day 6 compared to controls (P = 0 x 01). They also have a greater proliferation to allo-SP on both day 5 (P = 0 x 001) and day 6 (P = 0 x 01) at the same dilution. Using a stimulation index (SI) of 9 to either autologous SP or allo-SP on day 6 at the 1/50 dilution as a definition of a proliferative response to SP, then 13/20 patients as compared to 3/20 controls showed a proliferative response to SP (P = 0 x 003, Fishers exact test). These data support an autoimmune hypothesis for chronic prostatitis.
A Practical Guide to the Management of Prostatitis/Chronic Pelvic Pain Syndrome by Prof. J. Curtis Nickel. Förlag Bladon Medical Publishing in Oxfordshire, UK. Tfn: (01608) 644436, 12, New St, Chipping Norton, OX7 5LJ, United Kingdom. Pris cirka £25. ISBN: 1904218083 (Published May 2002). Utdrag ur boken och visst bildmateriel finns på följande URL: http://www.prostatitis.org/bookorder.html Citat från sidan 8: "Most [urologists] will concede that empiric treatment, practised by the majority of urologists, is ill-conceived and in many instances ineffective. The level of frustration among urologists dealing with prostatitis patients is evident. Given a choice, many urologists would decline to see these patients and many refuse to see patients again once they fail their initial prescription. Urologists have rated prostatitis the most difficult and frustrating disease entities that they manage." Citat från sidan 4, 5: "The effect of this particular disease, syndrome, or constellation of symtoms on a patient's quality of life can be accurately estimated and compared to the diseases for which quality of life and impact have been determined. When such comparisons are made, it becomes evident that the quality of life of a patient with chronic prostatitis is dismal. It is comparable to patients who have just had an acute myocardial infarction, or suffer from unstable angina, active Chron's disease, congestive heart failure or severe diabetes mellitus. ........."
I
läroboken "Kirurgi för sjuksköterskor", ISBN 91-44-07405-1,
förlag Studentlitteratur, kan man på sidan 302 bl.a. läsa:
"Kronisk abakteriell prostatit är vanligen en okomplicerad sjukdom med
godartat kliniskt förlopp även om det är besvärande för patienten".
Detta påstående är vilseledande, vittnar om dåliga kunskaper i ämnet,
strider mot
vad som framförts vid olika internationella symposier och vad som skrivits
i ansedda internationella medicinska tidskrifter under de senaste åren. Att därför göra en sådan förenklad beskrivning av en sjukdom (hålla kvar vid gamla myter) och t.ex.kalla svåra smärtor för att de endast "är besvärande för patienten", är skandalöst. Att sprida en sådan vilseledande information i en lärobok för sjukvårdspersonal innebär, att de som söker vård för svåra smärtor p.g.a. kronisk prostatit troligtvis kommer att bli betraktade som kverulanter och inte trovärdiga. Genom åtskilliga telefonsamtal och mail från olika delar av landet, har vi fått reda på att det verkligen förhåller sig på det här viset.
Motions- & Idrottsskador och deras rehabilitering Jag har saxat följande ur boken "Motions- & Idrottsskador och deras rehabilitering" av Jon Karlsson, Roland Thomée, Lars Martinsson och Leif Swärd. © SISU Idrottsböcker och författarna 2003, 3:e upplagan. ISBN: 91-88940-11-X "Prostatit Sannolikt är inflammation i prostatan den diagnos som oftast förbises hos personer med ljumskbesvär. Prostatit kan ge liknande besvär som de flesta övriga sjukdomar i ljumskregionen på grund av fortledd smärta i ljumsken ("referred pain"). Diagnosen ställs med klinisk undersökning och palpation av prostatan via ändtarmen (per rektum) och säkerställs med urinodling. Prostatainflammation är ofta kronisk och leder i många fall till återkommande problem. Behandlingen är 6 veckors antibiotikakur kombinerad med inflammationshämmande medel. Risken för återfall är stor. Vid kronisk eller återkommande prostatit bör urolog tillfrågas."
The impact of chronic prostatitis/chronic pelvic pain syndrome on patients. McNaughton Collins M. General Medicine Division, Massachusetts General Hospital, 50 Staniford Street, 9th Floor, Boston, MA 02114, USA. Chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) is a common condition, affecting men of all ages. Since mortality and serious complications are extremely uncommon, CP/CPPS is primarily a quality-of-life disease, and, therefore, the patient's perspective is of paramount importance. As with other non-life threatening diseases, the goal of treatment is to maximize quality not quantity of life. Scientifically validated methods to measure patients' health related quality of life have been applied in other urological diseases such as benign prostatic hyperplasia and interstitial cystitis; the same process is now underway in the study of CP/CPPS. Recent studies have shown that CP/CPPS takes a substantial toll on physical and mental health. In addition to examining the health related quality of life of patients with CP/CPPS, future studies should address additional patient-centered outcomes, such as satisfaction with care and the economic burden of the illness, in order to allow a more comprehensive understanding of the impact of this condition on patients.
J Urol. 2008 Jan 18; : 18207189 (P,S,G,E,B,D) Rodney U Anderson, Elaine K Orenberg, Christine A Chan, Angie Morey, Veronica Flores Department of Urology, Stanford University School of Medicine, Stanford, California. PURPOSE: Abnormal regulation of the hypothalamic-pituitary-adrenal axis and diurnal cortisol rhythms are associated with several pain and chronic inflammatory conditions. Chronic stress may have a role in the disorder of chronic prostatitis/chronic pelvic pain syndrome related to initiation or exacerbation of the syndrome. We tested the hypothesis that men with chronic pelvic pain syndrome have associated disturbances in psychosocial profiles and hypothalamic-pituitary-adrenal axis function. MATERIALS AND METHODS: A total of 45 men with chronic pelvic pain syndrome and 20 age matched, asymptomatic controls completed psychometric self-report questionnaires including the Type A personality test, Perceived Stress Scale, Beck Anxiety Inventory and Brief Symptom Inventory for distress from physical symptoms. Saliva samples were collected on 2 consecutive days at 9 specific times with strict reference to time of morning awakening for evaluation of free cortisol, reflecting secretory activity of the hypothalamic-pituitary-adrenal axis. We quantified cortisol variations as the 2-day average slope of the awakening cortisol response and the subsequent diurnal levels. RESULTS: Men with chronic pelvic pain syndrome had more perceived stress and anxiety than controls (p <0.001). Brief Symptom Index scores were significantly increased in all scales (somatization, obsessive/compulsive behavior, depression, anxiety, hostility, interpersonal sensitivity, phobic anxiety, paranoid ideation, psychoticism) for chronic pelvic pain syndrome, and Global Severity Index rank for chronic pelvic pain syndrome was 93rd vs 48th percentile for controls (p <0.0001). Men with chronic pelvic pain syndrome had significantly increased awakening cortisol responses, mean slope of 0.85 vs 0.59 for controls (p <0.05). CONCLUSIONS: Men with chronic pelvic pain syndrome scored exceedingly high on all psychosocial variables and showed evidence of dysfunctional hypothalamic-pituitary-adrenal axis function reflected in augmented awakening cortisol responses. Observations suggest variables in biopsychosocial interaction that suggest opportunities for neurophysiological study of relationships of stress and chronic pelvic pain syndrome.
Psychological Problems in Young Men with Chronic Prostatitis-like Symptoms Scandinavian Journal of Urology and Nephrology, September 2002 , pages 296 - 301 J. H. Ku; Y. S. Jeon; M. E. Kim; N. K. Lee; Y. H. Park. Department of Urology, Military Manpower Administration, Taejeon, Korea. Abstract Objective: To take a different perspective in assessing young men with chronic prostatitis-like symptoms, this study was designed since few prospective studies are available to survey a population of young men. Material and Methods: One hundred and fifty men aged 20 years dwelling in the community were randomly selected. Chronic prostatitis-like symptoms were measured by the National Institutes of Health-Chronic Prostatitis Symptom Index and the selfreported scores for pain and urinary symptoms were used to identify chronic prostatitis-like symptoms. The psychological methods used were the Beck Depression Inventory, the State-Trait Anxiety Inventory, and the Bem Sex Role Inventory. A total of 87 men (a response rate 58%) completed self-administered questionnaires. Results: As the scores for pain and urinary symptoms increased, those for depression increased ( p < 0.001 and p = 0.01, respectively). However, the mean scores for state and trait anxiety were not different according to the scores for pain and urinary symptoms. The mean masculinity scores were not different according to the scores for pain but those were significantly different according to the scores of urinary symptoms ( p = 0.042). The mean femininity scores were not different according to the scores of pain and urinary symptoms. Conclusions: Our findings suggest that psychological factors, especially depression and weak masculine identity may be associated with an early stage of chronic prostatitis-like symptoms. Young men with chronic prostatitis-like symptoms also have psychological problems. Hela artikeln finns på http://www.informaworld.com/smpp/content~content=a713800696?words=prostatitis&hash=2387638923
Chronic prostatitis is an independent risk factor for erectil dysfunction Stanley Zaslau, Dale Riggs, Barbara Jackson, Stanley Kandzari, Morgantown, WV. Från American Urological Association (AUA)'s Conference in San Antonio, 2005. Chronic prostatitis is an independent risk factor for erectile dysfunction (ED), say these researchers, who based their conclusion on an Intenet-based and in-clinic survey of chronic prostatitis patients, healthy patients, and patients who had other urologic problems, including ED. The survey used was the Sexual Health Inventory for Men (SHIM). Patients with chronic prostatitis had significantly lower total scores and also lower confidence that they could keep an erection than other patients. Patients with prostatitis (mean age 41.5 years) were younger than those seen for other urologic complaints (mean age 51 years) and older than healthy controls (mean age 25 years). The researchers recommended that chronic prostatitis patients should be asked about and offered treatment for ED in addition to their chronic prostatitis. Från Uro Today: http://www.urotoday.com/prod/contents/confreport/article.asp?cat=confReport&sid=184&tid=398&aid=3573 Frågeformulär
beträffande Sexual Health Inventory for Men:
Association between sleep apnea and erectile dysfunction? August 7, 2006 In the Department of Urology, Weill Medical College, Cornell University, New York Presbyterian Hospital, New York, New York 10021, USA. Researchers Teloken PE, Smith EB, Lodowsky C, Freedom T, Mulhall JP investigated a possible link between sleep apnea and erectile dysfunction? They concluded: “Men presenting with symptoms consistent with Sleep Aapnea Syndrome have a significant risk of erectile dysfunction, and the correlation between the severity of sleep apnea and the severity of erectile dysfunction is strong.” The Prostatitis Foundation had previously reported a link between sleep apnea and frequent urination, especially during the night.
Komplicerad UVI: Då det finns struktuella eller funktionella avvikelser i urinvägarna. UVI hos män bör alltid betraktas som komplicerad, eftersom prostatan oftast är involverad. Från Referensmetodik del I. Infektionsdiagnostik, I 5 Urinvägsinfektioner. Utgiven av Smittskyddsinstitutet (2:a upplagan 2000), 171 82 Solna.
NIH to Study Common Prostate Condition - Unexplained Pelvic Pain is Hallmark. November
2, 1998 Men who have unexplained discomfort or pain
in the pelvic area or chronic abacterial prostatitis are needed for a 5-year,
$5.5 million study funded by the National Institute of Diabetes and Digestive
and Kidney Diseases. Although no one knows how many men have prostatitis, experts think it is the most common genitourinary ailment in men younger than age 50, and the chronic abacterial form for which there is no known cause and no diagnostic test or reliable treatment predominates. Prostatitis occurs in men of all ages and races and accounts for an estimated 2 million visits to doctors each year, according to a national survey. Abacterial prostatitis is a syndrome of pain in the genital area and lower back, usually accompanied by frequent and urgent urination. It can effectively chain severely affected men to their bathrooms. Other symptoms such as burning or pain during voiding or ejaculation vary widely and may come and go without warning. The walnut-sized prostate sits forward of the rectum, below the bladder and surrounding the urethra, the tube through which urine passes out of the body. "It's amazing to me that we can't reliably treat the majority of men who have prostatitis. We hope this study will help us do a better job diagnosing and treating these men in the future, but we recognize the road ahead will probably be quite unpredictable," said Leroy M. Nyberg Jr., Ph.D., M.D., NIDDK study director. Tel: (301) 594-7717 Email: ln10f@nih.govFrom November 9 through October 2001, six medical centers will recruit more than 600 men for the Chronic Prostatitis Cohort Study. This will be the first large, multicenter study designed to gather well-defined, detailed, clinical information on the condition and then use that base to test and evaluate new treatment strategies in the future. The study will document symptoms, possible risk factors, medical histories and treatments; test blood, prostate fluid, semen and urine; and explore possible relationships between chronic prostatitis, urethral and bladder inflammation and other chronic pelvic pain disorders. Results are anticipated after September 2002. Desperate for relief, many men with chronic prostatitis are driven sometimes far from home to expensive, unproven and often disappointing remedies. The often prescribed, powerful antibiotics and drugs to relax the muscles of the prostate, in fact, often fail. Earlier studies observed small numbers of patients over short periods and used varying definitions, so that results were unclear and not comparable between studies. Besides focusing on hundreds of patients over 3 years, doctors in this study are also testing a new working definition of chronic abacterial prostatitis developed by consensus by researchers, physicians and patients at an NIDDK workshop in 1995.
Tillbaka till Forskning (på sidan Prostatasjukdomar)
May. 12, 1997 Contact: Laurie Mchale, Media Relations Coordinator, University of Washington, Department of Urology, Seattle, USA. http://www.uwnews.org/article.asp?articleID=2893 The Paul G. Allen Foundation for Medical Research has committed $3.2 million for research at the University of Washington into the causes of and cures for prostatitis, a common but understudied infection of the prostate gland. The foundation will contribute approximately $552,000 annually for the next five years to underwrite research into prostatitis conducted by the UW School of Medicine's Department of Urology. The research is under the direction of Dr. Richard E. Berger, professor of urology. The balance of the funding will go toward laboratory renovations and equipment costs. The UW has already completed a number of significant research projects on prostatitis, funded by more than $1 million in earlier contributions from the Microsoft co-founder and philanthropist. UW President Richard L. McCormick expressed gratitude for the gift and cited the "remarkable support in many areas" that Paul Allen and the foundations he has created have provided at the University of Washington. "We are pleased to support the University's groundbreaking research efforts and we hope that in some significant way, our gift will help to conquer this disease," said Jody Allen Patton, executive director of the Allen Foundations. "Past financial support from the Allen Foundation has already made the UW the leader in prostatitis research," said Berger. "We have made many exciting discoveries that will offer benefits for men with chronic prostatitis. This generous new support will enable us to significantly broaden our efforts." Despite the prevalence of prostatitis, there has been limited research into the condition, which may be the most common urologic disease of young and middle-aged men. Research has focused on the other maladies of the prostate: benign prostatic hypertrophy (BPH or enlarged prostate) and prostate cancer. Many men with BPH have symptoms of prostatitis as well. Estimates are that up to 50 percent of men will experience symptoms of prostatitis in their lifetimes. Symptoms can be varied and severe, including genital and bladder pain, inflammation, urinary problems, and perhaps infertility. While it is often dismissed as a minor condition, the decline in quality of life with prostatitis is similar to that experienced with congestive heart failure, according to UW research. Prostatitis is frequently difficult to diagnose, and causes are usually not clear. The various bacteria known to cause it often become resistant to antibiotics. Research directions with the new funding will include studies of the microbiology and molecular biology of prostatic tissue, development of diagnostic tests and treatment protocols, studies of host resistance factors that may cause susceptibility to infection, epidemiologic studies, and studies to determine any relationships to BPH and prostate cancer. The Paul G. Allen Foundation for Medical Research promotes medical research in a variety of disciplines, including biochemistry, biomedical engineering, virology, immunology, cell and molecular biology, pharmacology and genetics.
Oct. 8, 2002 FOR IMMEDIATE RELEASE: University of Washington awarded $1 million grant from The Paul G. Allen Foundation for Medical Research. The University of Washington Department of Urology announced today that it has received a $1 million grant from The Paul G. Allen Foundation for Medical Research to support continuing research by Dr. Richard Berger on chronic pelvic pain in men. "The Foundation is committed to supporting important medical research which promotes and improves health care delivery to individuals in the Pacific Northwest," said Jody Patton, executive director of the six Paul Allen Foundations. "The University of Washington and Dr. Berger have demonstrated encouraging progress in their previous research, which will not only have a significant impact on the daily lives of many people in our communities, but can be leveraged in other health care facilities and by physicians across the country." This grant opens the opportunity for Dr. Berger's lab to advance more quickly in its studies of chronic pelvic pain. Already the lab has developed a working model of idiopathic prostatitis (disease of the prostate gland) from clinical experience and ongoing research concerning the causes of chronic pelvic pain syndrome, or CPPS. "This model explains many of the previously puzzling manifestations of the disease," Berger said. "Our findings so far indicate that prostatitis definitely involves a great deal more than the prostate. This grant will help us expand our research into this problem and possible solutions." Berger's research so far has shown that application of botulism toxin, marketed as Botox, significantly decreases pain and difficulty with urination in men diagnosed with prostatitis in cases where antibiotics have failed. Berger has demonstrated the presence of spinal chord sensitization for the first time, and indicated that this sensitization helps set up a cycle of increased pain sensitivity, muscle spasm and increased pain from mild stimuli. Additionally, Berger has shown that genetic and stress factors may increase the likelihood of developing chronic prostatitis. "Our studies have also led us to believe that the mechanism of the vicious cycle of prostatitis pain is applicable to many poorly understood pain syndromes in both men and women," Berger said. "We are deeply grateful to the Foundation for its enlightened support of this research program." The grant will be distributed over two years, at $500,000 per year. The Paul G. Allen Foundation for Medical Research supports innovative programs and research that promote health, prevent disease and improve practices and health-care delivery. Founded in 1988, The Paul G. Allen Foundation for Medical Research ­ one of six foundations that support the use of technology in advancing medical treatments is administered through Vulcan Inc. of Seattle.
Ett okänt "Post-Orgasmic Syndrome"? Friday April 12, 2002 AMSTERDAM (Reuters) - Tired and sweaty after sex? A Dutch doctor said on Friday he is studying a rare new syndrome among middle-aged men who complain of flu-like symptoms for up to a week after having an orgasm. Marcel Waldinger, head of the department of psychiatry and neurosexology at Leyenburg Hospital in the Hague, said he planned to publish a report on "post-orgasmic illness syndrome" in the U.S. Journal of Sex and Marital Therapy this month. Waldinger has seen five Dutch men in as many years in his surgery complaining of a range of flu-like symptoms, including a sore throat, sweating, extreme fatigue and eye irritation after sex. "Men developed influenza-like symptoms within minutes of having an orgasm. It is like having a serious flu. This happens as soon as they have an orgasm," said Waldinger. "It is a new syndrome or a syndrome which is old but has not been looked at properly." The syndrome could be a physical disorder caused by an allergic reaction or the immune system in direct response to the release of chemicals in the body after sex. The symptoms lasted between three and seven days, he said. "We know that during orgasm and ejaculation very specific compounds like hormones are released into the nervous system. One hypothesis is that they might have had an allergic reaction to one of those compounds," Waldinger said.
Allmänt om tjocktarmsbakterier Enligt forskningsrapporten "LGG · Summatim" (kan beställas gratis på 08-7255150) från den finska livsmedelskoncernen VALIO, har man hittills påträffat 400-500 arter bakterier i tjocktarm och avföring. Dessutom anges att den totala volymen anaeroba bakterier (bakterier som inte kan leve i syre) i det här sammanhanget är 100-1000 gånger större än volymen aeroba bakterier (bakterier som måste ha syre för att kunna leva). Forskningsmetoder, som grundar sig på genomet (bakteriernas arvsfaktorer) har visat, att det finns en stor mängd bakteriearter som ännu inte identifierats och som inte växer på de odlingssubstrat som används på dagens moderna laboratorier. För oss med kronisk prostatit är detta synnerligen intressanta uppgifter, eftersom EN av orsakerna till kronisk prostatit troligtvis är olika tjocktarmsbakterier. Man har i vissa studier konstaterat att cirka 80 % av alla UVI orsakas av olika stammar av kolibakterier. Att ev. odling av bakterier vid kronisk prostatit, med hänsyn till ovan nämnda siffror, nästan alltid enbart utföres för aeroba bakterier är därför minst sagt anmärkningsvärt.
Urinvägsinfektion orsakad av antibiotikaresistenta E. coli bakterier från djur Clinical Infectious Diseases January 15, 2005;40(2): 251-7 Urinary tract infections likely caused by tainted food. Between October 1999 and January 2000, a single strain of E. coli was discovered to be responsible for drug-resistant UTIs in university communities in California, Minnesota, and Michigan. Researchers studied nearly 500 specimens of E. coli obtained from non-human sources such as cows, turkeys, dogs, sheep, and water. They found that one-quarter of the specimens were microbiologically indistinguishable from comparable human strains of E. coli. A more refined test showed that, of the drug-resistant specimens, one from a cow had a 94 percent similarity to a UTI-causing human strain of E. coli. The researchers concluded that the cause of the outbreak was probably foodborne. Bacterial drug resistance due to unnecessary antibiotic usage is a growing problem in health care, according to many experts. "People just have to be more conscious of when to use antibiotics for which infections," said lead author Lee W. Riley, MD, of the University of California-Berkeley. "Sometimes the use of these drugs may not be necessary." However, when drug-resistant organisms originate in animals, "there's not much people can do" to combat the increasing drug resistance, he added. Instead, foodborne illnesses are best avoided by smart food preparation. "The consumer has to be aware that foods can be infected and has to be careful in preparing food" by cooking it thoroughly, Dr. Riley said. Contact: Steve Baragona,sbaragona@idsociety.org ,703-299-0412 Founded
in 1979, Clinical Infectious Diseases publishes clinical articles
twice monthly in a variety of areas of infectious disease, and is one of
the most highly regarded journals in this specialty. It is published under
the auspices of the Infectious Diseases Society of America (IDSA). Based
in Alexandria, Virginia, IDSA is a professional society representing more
than 7,700 physicians and scientists who specialize in infectious
diseases. E. coli is a bacterium commonly found in the intestines of man and animals. We need this bacteria to break down cellulose and it assists in the absorption of vitamin K, the blood-clotting vitamin. Informativa sidor om E. coli är:
Tuberkulös prostatit hos en tidigare frisk man Från dansk Ugeskrift for Laeger 2008;170(1-2):58 Dr. Peter-Martin Krarup, Dr. Zaza Kamper-Jørgensen & Dr. Solveig Øster. Sydvestjysk Sygehus Esbjerg, Urologisk Klinik og Klinik for Patologisk Anatomi, og Statens Serum Institut, Mykobakteriologisk Laboratorium. Prostatit är en vanligt förekommande sjukdom, men som sällan orsakas av Mycobacterium tuberkulos. I en dansk man som var under utredning för symtom från urinvägarna, visade prostatabiopsier granulomatös prostatit (kornformig inflammatorisk vävnadsförändring) med kaseösa nekroser (ostliknande vävnadsdöd) och syrefasta stavar. Patientens odlingskultur var positivt för M. tuberculosis i både urin och sputum (spott). Relevant antituberkulös behandling inleddes. Tuberkulos är fortfarande en viktig diagnostik, som man måste tänka på vid urologipatienter. Extrapulmonal manifestation (påvisbart utanför lungorna) kan vara initialsymptom på tuberkulos och brist på kännedom om sjukdomen hos den drabbade innebär att smittan kan föras vidare.
Allmänt om tjocktarmsbakterien Enterococcus faecalis Enterococcus faecalis är en Gram-positiv bakterie som normalt finns i tjocktamen. Är en av de vanligaste bakterier som orsakar nosokomial (sjukdom orsakad vid behandling på sjukhus) infektion. T.ex. vid användning av kateter.
NEW YORK, Jan. 17, 2006 (UPI) -- A U.S.-led team of scientists has deciphered the genome of the parasite causing the sexually transmitted disease trichomoniasis. The researchers' finding is expected to lead to improved diagnoses and treatment of the disease the World Health Organization says affects approximately 170 million people a year and is an under- diagnosed global health problem. The team, led by Jane Carolton, an associate professor of medical parasitology at New York University, took four years to decipher the large genome of the single-celled parasite Trichomonas vaginalis. "It is a nasty bug," said Carlton, who noted that, in women, the parasite latches onto the vaginal lining and forms tendril-like projections into the tissue. In men the parasite can cause urogenital infections such as urethritis and prostatitis. The bug's large genome has around 26,000 confirmed genes, which is on par with the human genome. There might also be an additional 34,000 unconfirmed genes, bringing the total gene count to around 60,000 --one of the highest gene counts of any organism in the microbe, animal or plant communities. The research that involved 66 scientists from 10 nations is detailed in the current issue of the Journal Science.
Penetrering av antibiotika i prostatan Chemotherapy, International Journal of Experimental and Clinical Chemoterapi. 2003 Dec;49(6):269-79. Penetration of antimicrobial agents into the prostate. In the present review article, the penetration of antimicrobial agents into prostatic fluid and tissue was examined. Three major factors determining the diffusion and concentration of antimicrobial agents in prostatic fluid and tissue are the lipid solubility, dissociation constant (pKa) and protein binding. The normal pH of human prostatic fluid is 6.5-6.7, and it increases in chronic prostatitis, ranging from 7.0 to 8.3. A greater concentration of antimicrobial agents in the prostatic fluid occurs in the presence of a pH gradient across the membrane separating plasma from prostatic fluid. Of the available antimicrobial agents, beta-lactam drugs have a low pKa and poor lipid solubility, and thus penetrate poorly into prostatic fluid, expect for some cephalosporins, which achieve greater than or equal to the inhibitory concentration. Good to excellent penetration into prostatic fluid and tissue has been demonstrated with many antimicrobial agents, including tobramycin, netilmicin, tetracyclines, macrolides, quinolones, sulfonamides and nitrofurantoin. Copyright 2003 S. Karger AG, Basel Hela artikeln finns att läsa på Penetration.pdf - Från Chemoterapi 2003;49:269-279 angående antibiotikas penetrering i prostatakörteln. Originalartikeln
finns på http://content.karger.com/ProdukteDB/produkte.asp?Aktion=ShowFulltext&Produkt
A Theory why Antibiotics Don`t work During infection the prostate tries to circumscribe the infected area by surrounding it with a polysaccharide shield which cannot be penetrated by antibiotics that are administered systemically. Bacteria exist inside the infected, obstructed calculi and acini which cannot be reached by antibiotics and which become the source of recurrent infection. In patients with long-term chronic prostatitis T-cells, which are reactive to normal prostatic protein, are frequently detected (Alexander, 1977). Levels of cytokines such as IL2, IL6 and TNF alpha in the sperm of these patients were much higher than normal, suggesting prostatitis may be, or may become, an autoimmune disease.
Allmänt om "prostataförkalkningar" Eur Urol. 2004 Mar;45(3):333-7; discussion 337-8. Clinical correlation of prostatic lithiasis with chronic pelvic pain syndromes in young adults. Geramoutsos I, Gyftopoulos K, Perimenis P, Thanou V, Liagka D,Siamblis D, Barbalias G. Department of Urology, Mesolongi General Hospital, Mesolongi, Greece. OBJECTIVE: To investigate the incidence, morphology and clinical presentation of prostatic calculi in a selected population of young adults and to examine any possible correlation with chronic prostatitis/chronic pelvic pain syndromes (CP/CPPS). METHODS: A population of 1374 young adults was screened with ultrasound imaging of the prostate and 101 cases with prostatic lithiasis were selected. Patients were divided in two groups, according to the type of prostatic calculi (type A: small, multiple or type B: larger, coarser calculi). Further evaluation included history and physical examination, recording of lower urinary tract symptoms and theMeares-Stamey test. RESULTS: Calculi were type A in 71.3% and type B in 28.7% of cases. Localization (central/periurethral) was not correlated with other parameters. Age was closely related to calculus burden ( p =0.034 ). Type B calculi were more often associated with symptoms and chronic prostatitis/CPPS (chi(2)-test, p=0.007 and 0.018 respectively). CONCLUSIONS: Small, multiple calcifications are a normal, often incidental ultrasonographic finding in the prostate and represent a result of age rather than a pathologic entity. However, larger prostatic calculi may be related to underlying inflammation and require further evaluation and possibly, treatment.
Från Dr. Daniel Skoskes http://www.dshoskes.com/cpclinic.html "The role of prostatic stones in producing the symptoms of prostatitis is controversial, especially since many older men without symptoms are found to have these stones. Nevertheless, younger men with extensive prostatic calcification are often improved when these stones are eliminated. We have a limited but very positive experience treating these men with combination therapy against nanobacteria, a type of stone forming bacteria impossible to detect using typical culture techniques.Therapy consists of a daily antibiotic (tetracycline), an oral supplement and an EDTA rectal suppository and typically lasts 3 months."
Aravantinos E, Kalogeras N, Zygoulakis N, Kakkas G, Anagnostou T, Melekos M. Department of Urology, University of Thessaly, School of Medicine, Larissa, Greece. BACKGROUND AND PURPOSE: A novel approach for continuous drainage of prostatic abscesses is presented and discussed. PATIENTS AND METHODS: We present seven cases diagnosed with prostatic abscess during 2001-2007. The diagnosis was based on either clinical or transrectal ultrasound (TRUS) findings. All patients were initially treated as prostatitis cases by intravenous antibiotics, a1 blockers, and a suprapubic catheter. Those diagnosed with an abscess had a drainage tube placed transrectally under TRUS guidance, and it was left in place for 24-36 hours. RESULTS: Past medical history most often included previous urinary infection (n = 4), bladder outlet obstruction (n = 1), and diabetes mellitus (n = 4). In all patients, prostatic abscess was greater than 1.5 cm, and in two patients the abscess was multifocal. All abscesses were completely resolved by transrectal continuous drainage, and the average hospitalization period was 10 days. No patient required a second intervention. All patients received antibiotics for 1 month following the procedure. CONCLUSION: Although rare, prostatic abscess is a serious condition that needs quick diagnosis and treatment. In our experience, TRUS-guided transrectal placement of a drainage tube is a feasible and safe treatment alternative for prostatic abscess; it is also easy to perform and well tolerated by the patients. PMID: 18673079 [PubMed - in process]
Botox might shrink swollen prostateThursday, September 01, 2005 By Byron Spice, Pittsburgh Post-Gazette Botox is perhaps best known for reducing facial wrinkles, but University of Pittsburgh physicians say it can also reduce the size of a man's enlarged prostate gland. One injection of the botulinum toxin can shrink the prostate for six to nine months, providing relief from symptoms that increase the frequency and the difficulty of urination in men. "It's definitely not ready for prime time," emphasized Dr. Michael Chancellor, a Pitt urologist who yesterday presented findings from animal studies and from a small clinical trial in Taiwan at the International Continence Society meeting in Montreal. "But it's intriguing," he added, noting he offers this "off-label" use of Botox for UPMC patients who aren't adequately helped by conventional treatments. Larger studies to demonstrate the treatment's safety and effectiveness will be necessary before it is likely to spread beyond the relative handful of urologists who now offer the treatment, said Chancellor, who is seeking a federal grant for such a study. Allergan Inc., the maker of Botox, says it plans to launch its own U.S. clinical trial by the end of the year. An estimated 6 million men have enlarged prostates, a condition that becomes more common as men grow older. About a third of all men over age 75 have some degree of prostate enlargement. It is distinct from prostate cancer, another common disease in men. Benign prostatic hyperplasia occurs as the prostate gland grows bigger with age and starts to impinge on the urethra, which carries urine from the bladder. Men with enlarged prostates may feel the need to urinate more frequently and may have more difficulty starting and stopping the urine flow. Botulinum toxin type A has found a number of uses as a muscle relaxant since it was first approved by the FDA in 1989 for treating eye muscle disorders. But the mechanism by which Botox works in prostatic disease is a bit different, Chancellor said. As reported yesterday, injections into the prostates of laboratory rats showed that the toxin induced apoptosis, or programmed cell death, in some of the prostate cells, helping to reduce the size of the gland. The injections also made the glands less sensitive to the hormone epinephrine and similar substances, which cause the prostate and bladder muscles to tighten up. The walnut-size gland surrounds the urethra, so when the gland contracts it can be difficult to void urine. Botox allows the gland to relax, improving flow. "The drug can treat prostate problems when the pills don't work because we can alter how body chemicals talk to the prostate," Chancellor said. Surgery can be effective in treating severe symptoms, though the operation includes a small risk of bleeding, infection and impotence. Drugs such as Proscar and Avodart can block hormones that cause the gland to enlarge, but they don't work for all men. A family of high blood pressure medications, known as alpha blockers, also can reduce symptoms, but again are not always effective. Chancellor and his Taiwan colleagues are presenting findings from 16 patients treated in the Taiwanese clinical trial. He said he also has treated UPMC patients who do not want surgery and have not been helped by the conventional drugs. But the number of patients treated remains small, around 50. The technique itself is simple, he noted, and is much the same as would be used to do a biopsy of the prostate. Från http://www.post-gazette.com/pg/05244/563456.stm Post-Gazette science editor Byron Spice can be reached at bspice@post-gazette.com or 412-263-1578.
Saw palmetto no aid to prostate health US researchers carried out a year-long study of 225 men, none of whom knew if they were taking the real herb or not. Men report anecdotally that they find saw palmetto helps with their symptoms. Having an enlarged prostate - also known as benign prostate hyperplasia (BPH) - is very common, affecting about one third of men over 50. No difference. The US research was carried by doctors at the San Francisco VA Medical Center and the Northern California Kaiser Permanente Division of Research. Patients, who all had enlarged prostates - were randomly assigned to take either the herbal extract or the dummy pill twice a day. They were assessed regularly to see if there had been any change in their condition, or in urinary function. Dr Stephen Bent, who led the research, said: "If you look at the change in symptoms over time between the two groups, it was almost identical. "There was no statistically significant difference at any time point during the study." The researchers also looked at particular groups of patients, comparing those with more and less severe symptoms and those with larger and smaller prostates - but found no difference in any of the subgroups between the herbal extract and the dummy version. Dr. Bent added: "The results of this study clearly do not support a strong clinical benefit of saw palmetto." But he said it was possible other groups of patients might respond differently to the herbal extract. He said the findings of this study did contradict earlier research. However, he said: "Prior studies were generally small in size and short in duration. Plus, the vast majority of them did not use the standard symptom score that we used for assessing the severity of BPH." He said also it had also previously been difficult to mimic the distinctive and strong smell and taste of saw palmetto - making it easier for patients to know during the study whether or not they are taking the real thing. Dr. Debbie Clayton, head of information at the UK's Prostate Cancer Charity, said: "This is an interesting study because it contradicts the findings of previous studies. "We await the results of future trials to see if these results can be duplicated. "We also need to see the effect of higher doses studied. The doses available from high street shops in the UK are higher than those used in this study." She added: "Men report anecdotally that they find saw palmetto helps with their symptoms of BPH. "We would advise men who are considering taking saw palmetto to discuss this with their doctor first, especially as it can mask a man's true PSA l[prostate specific antigen] level. "We would also advise men to be aware that saw palmetto does not prevent prostate cancer."
Likheter mellan manliga och kvinnliga könsorgan Okänd källa. But, of course, it's an illusion. Those diametrically opposed concepts, such as male and female, are merely expressions of the same thing. Every male has a uterus called utricle, however small and under developed it may be. Ovaries and testicles are the same organ with slightly different functions. Prostate gland and Skenes gland are the same gland, as are Cowpers glands and Bartolin glands. Clitoris and penis are the same, they simply are of different sizes and names. Even the biochemical's that determine reproductive gender, testosterone and estrogen are the same chemical, built on a steroid nucleus (perhydrocyclopentaphenanthren), save for the presence of a single hydrogen atom at a particular place on the molecule. The point being made is that female and male are not as opposite as formerly considered. Therefore, isn't out of reach, but becomes transitional roadmap for reality change in the face of an illusion of impossibility.
Vi "jagar" intressanta artiklar!
|