|
Diagnostik och behandling av kronisk prostatit
Dr. Bruno Dahlberg Med. Dr. Docent. Avled 2003.
En ny behandlingsmetod för kronisk prostatit Den kroniska prostatit som drabbar både unga och medelålders beror på en sjukdom i prostatakörteln. För en diagnos måste ett prov från prostatakörteln erhållas. Detta kan ske på det vanligaste sättet med massage av prostatakörteln och undersökning av sekretet med mikroskopering av det s.k. exprimatet eller försök till odling. En odling av bakterier kan bli negativ d.v.s. ingen växt. Detta beror sannolikt på att ingen frågar efter när senaste sädesutlösning var. De närmaste 4 dagarna efter en sådan är risken för en falskt negativ reaktion. Efter en abstinens på 5 dagar eller fler ökar antal positiva odlingar till över 80-90 %. En ny metod som har brukats på vår klinik i många är följande: För att få ut tillräckligt med sekret från prostata så är en sädesuttömning nödvändig. Säden består av spermier samt rikligt med prostatasekret och kallas för spermieprovet. Avhållsamhetstiden eller abstinenstiden är avgörande för om ett prov skall visa bakterier eller ej. Bakterieodlingen avläses efter 5-6 dagar. Typ av bakterier kan variera men är mestadels bakterier som återfinns i tjocktarmen. Av större intresse är vilken typ av antibiotika kan användas i varje enskilt fall. Den andra undersökningen som sker är prostataundersökning med massage. Härvid kan dels direktprov tas d.v.s. att det droppar sekret från prostata på ett glas för direkt mikroskopi. Dessutom tas urinprov som centrifugeras och mikroskoperas för observation av antal vita blodkroppar, bakterier och svamp. Att en sjukdom är kronisk betyder inte att den är obotlig. Däremot är risken för återfall stor. Behandling: Antibiotika ges först med provdos för att utesluta allergiska reaktioner, därefter sker långtidsbehandling som kan ta från 3-4 månader till 24 eller 36 månader eller längre. Behandlingen pågår till patienten känner sig frisk. Byte av antibiotika kan även ske efter 5-6- månaders behandling för att få optimal effekt. Detta kontrolleras med en ny odling.. Man blir inte immun mot ett preparat men effekt kan minska. Om även spermieodlingarna blir normala och prostataproven normala så kan patienten då vara frisk. Tilläggsbehandling är Selen 1 mg (?) dagligen som är en stark antioxidant och skyddar prostata enligt modern forskning mot prostatacancer. Som är välkänt är att även en lindrig nedkylning av prostataområdet kan få återfall. Detta gäller även nedkylning av fötter och lår. Prostatamassage botar inte sjukdomen men avhjälper besvär. Samma sak med varma sittbad. Resultat: På 400 behandlade fall har 95 % blivit "normala". Abakteriell prostatit förekommer endast i 2 %. 5 % återkom ej efter första besöket, möjligen beroende på långa reseavstånd. En patient kan vara frisk i månader eller år beroende på om dom undviker nedkylningseffekten.
Hypertension in males with prostatitis. Från Advance in Reproduction, Vol IV, Issue 2,3. June 2000. When investigating male infertility connected with silent genital infection - Asymptomatic bacteriospermia (- ABS) there are cases with ABS combined and hypertension. (Dahlberg, 1976; 2000). The etiology of hypertension is still an enigma and in 95% of cases the cause is unknown. Bacteriuria develops in a hypertensive populations as shown in a seven-year study (Shapiro et al, 1971) and blood pressure was lowered in non-infected patients but treatment of the bacteriuria and its correlation with hypertension/blood pressure was not performed. In a multiphasic screening program, bacteriuria and hypertension were studied but no correlation was found (Takala et al, 1979). The purpose of this study was to explore if a correlation exists between genital infection in men and hypertension in men, and to investigate if the treatment of the infection had an effect on the hypertension. Of the men examined at the clinic, (17 %) of the men had asymptomatic prostatitis i.e. partners of women with repeated Urinary Tract Infections (UTI). Materials/Methods: 243 men 22-60 years of age (mean 44 years) were examined.. The asymptomatic group of 40 cases (17 %) were partners of women who had recurrent Urinary Tract Infection (UTI) for more than three times in a period of four months where no other cause of the UTI was apparent. They agreed to have an andrologic examination. Symptomatic cases were 203 men. The usual symptoms of chronic and sub chronic prostatitis were: Dysuria, nocturia, pain in the genital region, pain of muscles and joints, back pain, mental and physical fatigue, loss of libido and impotence and painful ejaculations. None of the men took drugs for hypertension. For controls, 936 men (40-44 years) were screened for blood pressure (BP). In Malmö city, 174 (19 %) had a BP 0140/90. (Peter Nilsson, Personal communication Research Centre, University Hospital, Malmö). The culture of microbes in spermtests for bacteriospermia (Dahlberg, 1976; Derrick/Dahlberg, 1976) was combined with expressed prostatic fluid examination (Ludvig et al, 2000). After urinating and washing the glans penis the men delivered a spermtest. Prostate gland examination and gland massage was done. To obtain optimum results of five day coital abstinence was important for cultures of spermtests to detect bacteriospermia (Dahlberg 1976; Derrick, Dahlberg 1976) and expressed prostatic secretions (Dahlberg 2000), (fig 1). The importance of the period of abstinence is shown in table 1. Positive cultures were sensitivity tested to indicate the preferable treatment. No cultures were done on prostatic secretions. In 98 cases the patient volunteered a spermtest. Evaluation of cultures: Negative = no growth. Postive = growth. Prostatic secretions: Positive >- 10 White Blood Cells per High Power Field = (WBC/HPF). Hypertension was defined as: >- 140/90 mm Hg. Blood pressure was measured with Hg manometer with the patient in recumbent position and after 10 minutes of rest. Patients were asked about the heredity background of hypertension status of their parents. Results/Discussion: Spermtests were delivered in 98 cases (40 %). In 95 cases (98 %) there were positive cultures. In three cases the cultures were negative but expressed prostatic secretion (EPS) test were positive. EPS was done in 239 cases, four refused the examination but delivered spermtests that showed bacteriospermia. Of the 239 examined men 235 (98 %) had >40 WBC/HPF with a range of 10-500 WBC/HPF. Hypertension was found in 115 cases (47 %). Range 140/90 - 210/120. Known heredity cause was found in 27 cases (25 %). Antibacterial agents used were if possible according to Sensitivity tests (Trimethoprim, Doxacyclin, Pivampicillin, Norfloxacin). Pathogens were not accounted for. The time of treatment to normalize blood pressure (BP): Ranged from 1-9 months (mean 3.4). Normalized BP was found in 115 (98 %). In two cases the BP was lowered but not under 140/90. Genital infection in men is a well-known ailment and is treated in different ways. Hypertension is a well-defined symptom and according to specialists in hypertension the cause is unknown in 95% of the cases. This study was conducted to investigate both sperm cultures and expressed prostatic secretions from the same patient. There were 98 spermtests delivered (40 %) with cultures done. The majority of patients (60 %) declined a sperm test due to various reasons: Difficulty to masturbate in a Clinic, sexual inadequacy, loss of libido, impotence an/or painful ejaculations. Prostatic examination was done in 239 cases with four declining but delivering spermtests. All men were treated with antibacterial agents. In the 40 (17 %) asymptomatic males where the female partner had repeated UTI - hypertension was found in 20 men (50 %). In the total population 115 (47 %) had hypertension. Comparison with the control group of 936 men aged 40-44 years where there was hypertension in 174 (19 %) shows a significant difference with 47 % of cases with genital infections 15 of the patients with hypertension had taken blood tests for cholesterol/serum on their own initiative. They were all elevated at the beginning of the study. Blood pressures and cholesterol values were normalized after treatment. The patients with hypertension were advised to return subsequently to the Clinic if their blood pressure tended to rise. There is no explanation for the connection between infection and hypertension. There might be a reaction in the whole body possibly an antibody reaction related to autoimmune diseases. Antibacterial treatment had no negative effects on patients. All patients with prostatitis felt better with alleviation of symptoms. Antibacterial treatment of genital infection may reduce blood pressure (BP). Usually the hypertensive patient is treated with lifelong medications. The relatively short period of treatment was welcomed by the patients and even if this is one of the causes of hypertension it may be a source of problems for the doctor. It is easier for an andrologist or urologist to measure B.P. and administer medication than it is for an internist to examine a patient for genital infection. Prostatitis/hypertension was found in 47 % of the men and in a relatively short time of antibacterial treatment all but two men had normalized blood pressure. The method was well accepted by the patients and their genital infection symptoms were alleviated.
Table of microscopy of prostatitis secretion in 100 men, expressed in White Blood Cells (WBC) per High Power Fields (HPF)
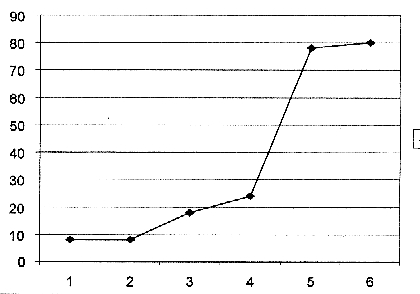
Days of abstinence= period of incubation Figure 1: Significance of period of abstinence for detection of bacteriospermia in 60 cases (10 cases per dot each).
References: Dahlberg B. (1976): Asymptomatic bacteriospermia. Cause of infertility In men. Urology 8:563-566. Dahlberg B. (2000): Hypertension in infertile males-caused by Asypmtomatic bacteriospermia. Conference, Jena, Germany. Derrick FC., Dahlberg B.(1976): Male genital tract infections and sperm viability. In Hafez Human semen and fertility regulation in men. St Louis: Mosby, pp389-392. Ludwig M., Schroeder-Printzen I., Ludecke G., Weidner M. (2000): Comparision of expressed prostatic secretions with urine after prostatic massage. Urology55:175-177. Shapiro AP., Sapira JD., Scheib ET.(1971): Development of bacteriuria in a hypertensive population. AnnIntern Med74:861-868 Takala J.,Sievers K.,Takala A. (1979): Multiphasic screening program at the Health Centre level. The Säkylä-Köylio project Scand J Sic Med 7:87-91
Tillbaka till Diagnos (På sidan Prostatasjukdomarna)
|